

Clinicopathologic Features and Magnetic Resonance Imaging Findings in 24 Cats With Histopathologically Confirmed Neurologic Feline Infectious Peritonitis
- PMID: 28833469
- PMCID: PMC5598904
- DOI: 10.1111/jvim.14791
Clinicopathologic Features and Magnetic Resonance Imaging Findings in 24 Cats With Histopathologically Confirmed Neurologic Feline Infectious Peritonitis
Abstract
Background: Feline infectious peritonitis (FIP) is the most common infectious central nervous system (CNS) disease in the cat and is invariably fatal. Improved means of antemortem diagnosis is required to facilitate clinical decision making. Information regarding the magnetic resonance imaging (MRI) findings of neurologic FIP currently is limited, resulting in the need for better descriptions to optimize its use as a diagnostic tool.
Objective: To describe the clinicopathologic features and MRI findings in cases of confirmed neurologic FIP.
Animals: Twenty-four client-owned cats with histopathologic confirmation of neurologic FIP.
Methods: Archived records from 5 institutions were retrospectively reviewed to identify cases with confirmed neurologic FIP that had undergone antemortem MRI of the CNS. Signalment, clinicopathologic, MRI, and histopathologic findings were evaluated.
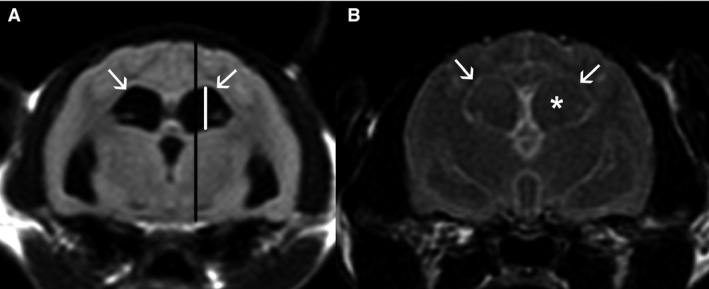
Results: Three distinct clinical syndromes were identified: T3-L3 myelopathy (3), central vestibular syndrome (7), and multifocal CNS disease (14). Magnetic resonance imaging abnormalities were detected in all cases, including meningeal contrast enhancement (22), ependymal contrast enhancement (20), ventriculomegaly (20), syringomyelia (17), and foramen magnum herniation (14). Cerebrospinal fluid was analysed in 11 cases; all demonstrated a marked increase in total protein concentration and total nucleated cell count. All 24 cats were euthanized with a median survival time of 14 days (range, 2-115) from onset of clinical signs. Histopathologic analysis identified perivascular pyogranulomatous infiltrates, lymphoplasmacytic infiltrates, or both affecting the leptomeninges (16), choroid plexuses (16), and periventricular parenchyma (13).
Conclusions and clinical importance: Magnetic resonance imaging is a sensitive means of detecting neurologic FIP, particularly in combination with a compatible signalment, clinical presentation, and CSF analysis.
Keywords: Feline infectious peritonitis; Histopathology; Magnetic resonance imaging; Neurologic.
Copyright © 2017 The Authors. Journal of Veterinary Internal Medicine published by Wiley Periodicals, Inc. on behalf of the American College of Veterinary Internal Medicine.
Figures




References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
