

Guided bone regeneration: materials and biological mechanisms revisited
- PMID: 28833567
- PMCID: PMC5601292
- DOI: 10.1111/eos.12364
Guided bone regeneration: materials and biological mechanisms revisited
Abstract
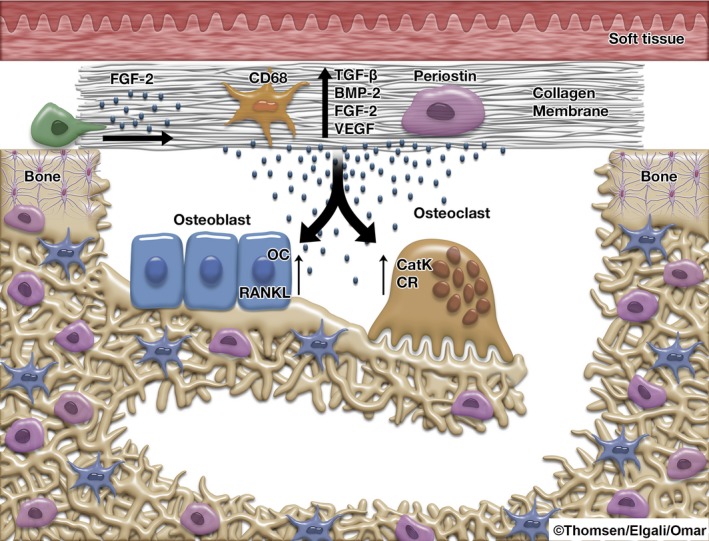
Guided bone regeneration (GBR) is commonly used in combination with the installment of titanium implants. The application of a membrane to exclude non-osteogenic tissues from interfering with bone regeneration is a key principle of GBR. Membrane materials possess a number of properties which are amenable to modification. A large number of membranes have been introduced for experimental and clinical verification. This prompts the need for an update on membrane properties and the biological outcomes, as well as a critical assessment of the biological mechanisms governing bone regeneration in defects covered by membranes. The relevant literature for this narrative review was assessed after a MEDLINE/PubMed database search. Experimental data suggest that different modifications of the physicochemical and mechanical properties of membranes may promote bone regeneration. Nevertheless, the precise role of membrane porosities for the barrier function of GBR membranes still awaits elucidation. Novel experimental findings also suggest an active role of the membrane compartment per se in promoting the regenerative processes in the underlying defect during GBR, instead of being purely a passive barrier. The optimization of membrane materials by systematically addressing both the barrier and the bioactive properties is an important strategy in this field of research.
Keywords: biocompatible materials; growth factors; guided bone regeneration; membrane; osseointegration.
© 2017 The Authors. Eur J Oral Sci published by John Wiley & Sons Ltd.
Figures
References
-
- Chiapasco M, Zaniboni M, Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res 2006; 17(Suppl): 136–159. - PubMed
-
- Bernstein S, Cooke J, Fotek P, Wang HL. Vertical bone augmentation: where are we now? Implant Dent 2006; 15: 219–228. - PubMed
-
- Donos N, Mardas N, Chadha V. Clinical outcomes of implants following lateral bone augmentation: systematic assessment of available options (barrier membranes, bone grafts, split osteotomy). J Clin Periodontol 2008; 35: 173–202. - PubMed
-
- Rocchietta I, Fontana F, Simion M. Clinical outcomes of vertical bone augmentation to enable dental implant placement: a systematic review. J Clin Periodontol 2008; 35: 203–215. - PubMed
-
- Hammerle CH, Jung RE. Bone augmentation by means of barrier membranes. Periodontol 2000 2003; 33: 36–53. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
