

Cost-Effectiveness of Intensive versus Standard Blood-Pressure Control
- PMID: 28834469
- PMCID: PMC5708850
- DOI: 10.1056/NEJMsa1616035
Cost-Effectiveness of Intensive versus Standard Blood-Pressure Control
Abstract
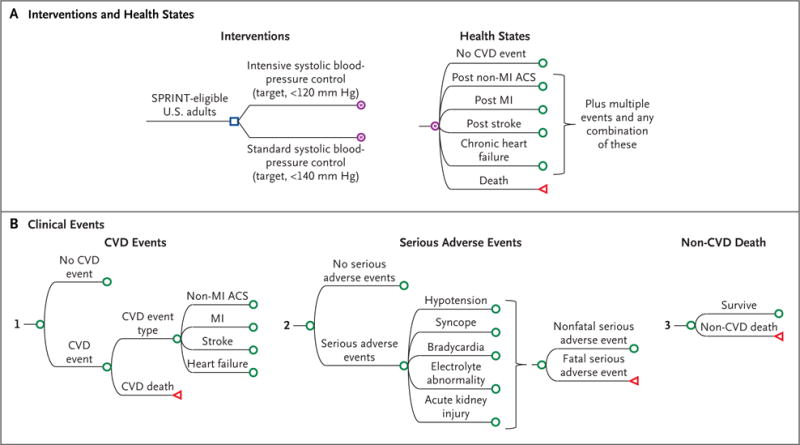
Background: In the Systolic Blood Pressure Intervention Trial (SPRINT), adults at high risk for cardiovascular disease who received intensive systolic blood-pressure control (target, <120 mm Hg) had significantly lower rates of death and cardiovascular disease events than did those who received standard control (target, <140 mm Hg). On the basis of these data, we wanted to determine the lifetime health benefits and health care costs associated with intensive control versus standard control.
Methods: We used a microsimulation model to apply SPRINT treatment effects and health care costs from national sources to a hypothetical cohort of SPRINT-eligible adults. The model projected lifetime costs of treatment and monitoring in patients with hypertension, cardiovascular disease events and subsequent treatment costs, treatment-related risks of serious adverse events and subsequent costs, and quality-adjusted life-years (QALYs) for intensive control versus standard control of systolic blood pressure.
Results: We determined that the mean number of QALYs would be 0.27 higher among patients who received intensive control than among those who received standard control and would cost approximately $47,000 more per QALY gained if there were a reduction in adherence and treatment effects after 5 years; the cost would be approximately $28,000 more per QALY gained if the treatment effects persisted for the remaining lifetime of the patient. Most simulation results indicated that intensive treatment would be cost-effective (51 to 79% below the willingness-to-pay threshold of $50,000 per QALY and 76 to 93% below the threshold of $100,000 per QALY), regardless of whether treatment effects were reduced after 5 years or persisted for the remaining lifetime.
Conclusions: In this simulation study, intensive systolic blood-pressure control prevented cardiovascular disease events and prolonged life and did so at levels below common willingness-to-pay thresholds per QALY, regardless of whether benefits were reduced after 5 years or persisted for the patient's remaining lifetime. (Funded by the National Heart, Lung, and Blood Institute and others; SPRINT ClinicalTrials.gov number, NCT01206062 .).
Figures


Comment in
-
Cost-Effectiveness of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2017 Nov 30;377(22):2199. doi: 10.1056/NEJMc1712465. N Engl J Med. 2017. PMID: 29188982 No abstract available.
References
-
- James PA, Oparil S, Carter BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8) JAMA. 2014;311:507–20. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical