

Voriconazole-refractory invasive aspergillosis
- PMID: 28835093
- PMCID: PMC5583461
- DOI: 10.3904/kjim.2017.109
Voriconazole-refractory invasive aspergillosis
Abstract
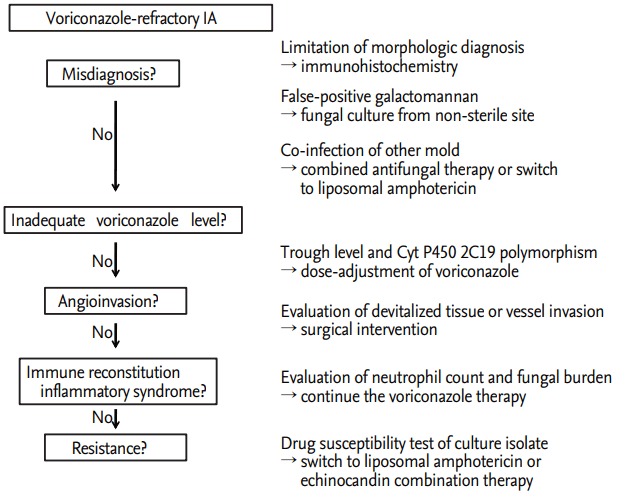
Invasive aspergillosis (IA) is one of the most common life-threatening complications in immunocompromised patients. Voriconazole is currently the drug of choice for IA treatment. However, some patients with IA suffer clinical deterioration despite voriconazole therapy. Management of voriconazole-refractory IA remains challenging; no useful recommendations have yet been made. Voriconazole-refractory IA can be further categorized as disease attributable to misdiagnosis or co-infection with another mold; inadequate blood voriconazole blood; inadequate tissue drug concentrations attributable to angioinvasion; immune reconstitution inflammatory syndrome; or infection with voriconazole-resistant Aspergillus. Hence, when encountering a case of voriconazole-refractory IA, it is necessary to schedule sequential tests to decide whether medical treatment or surgical intervention is appropriate; to adjust the voriconazole dose via drug monitoring; to seek CYP2C19 polymorphisms; to monitor serum galactomannan levels; and to examine the drug susceptibility of the causative Aspergillus species.
Keywords: Aspergillosis; Aspergillus; Immunocompromised host; Therapy; Voriconazole.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Invasive Aspergillus infection requiring lobectomy in a CYP2C19 rapid metabolizer with subtherapeutic voriconazole concentrations.Pharmacogenomics. 2016 May;17(7):663-7. doi: 10.2217/pgs-2015-0014. Epub 2016 May 4. Pharmacogenomics. 2016. PMID: 27143031
-
Invasive pulmonary aspergillosis due to azole-resistant Aspergillus lentulus.Pediatr Int. 2017 Mar;59(3):362-363. doi: 10.1111/ped.13193. Pediatr Int. 2017. PMID: 28317305 No abstract available.
-
Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline.Clin Microbiol Infect. 2018 May;24 Suppl 1:e1-e38. doi: 10.1016/j.cmi.2018.01.002. Epub 2018 Mar 12. Clin Microbiol Infect. 2018. PMID: 29544767
-
Invasive pulmonary aspergillosis due to Aspergillus lentulus in an adult patient: A case report and literature review.J Infect Chemother. 2019 Jul;25(7):547-551. doi: 10.1016/j.jiac.2019.02.003. Epub 2019 Feb 26. J Infect Chemother. 2019. PMID: 30824299 Review.
-
Interpersonal Factors in the Pharmacokinetics and Pharmacodynamics of Voriconazole: Are CYP2C19 Genotypes Enough for Us to Make a Clinical Decision?Curr Drug Metab. 2018;19(14):1152-1158. doi: 10.2174/1389200219666171227200547. Curr Drug Metab. 2018. PMID: 29361899 Free PMC article. Review.
Cited by
-
Fungal brain infection-no longer a death sentence.Neurosurg Rev. 2021 Aug;44(4):2239-2244. doi: 10.1007/s10143-020-01410-3. Epub 2020 Oct 9. Neurosurg Rev. 2021. PMID: 33037537 Free PMC article.
-
Disseminated cerebral aspergillosis complicated by thrombotic microangiopathy.Med Mycol Case Rep. 2019 Jul 5;25:25-28. doi: 10.1016/j.mmcr.2019.07.002. eCollection 2019 Sep. Med Mycol Case Rep. 2019. PMID: 31334000 Free PMC article.
-
Trends on Aspergillus Epidemiology-Perspectives from a National Reference Laboratory Surveillance Program.J Fungi (Basel). 2021 Jan 6;7(1):28. doi: 10.3390/jof7010028. J Fungi (Basel). 2021. PMID: 33418997 Free PMC article.
-
Invasive Aspergillosis after Renal Transplantation.J Fungi (Basel). 2023 Feb 15;9(2):255. doi: 10.3390/jof9020255. J Fungi (Basel). 2023. PMID: 36836369 Free PMC article. Review.
-
Invasive cerebral aspergillosis in a pregnant woman: a rare case of intracranial giant granuloma.BMC Infect Dis. 2025 Apr 8;25(1):478. doi: 10.1186/s12879-025-10884-9. BMC Infect Dis. 2025. PMID: 40200155 Free PMC article.
References
-
- Kim SH, Moon SM, Han SH, et al. Epidemiology and Clinical outcomes of invasive pulmonary aspergillosis: a nationwide multicenter study in Korea. Infect Chemother. 2012;44:282–288.
-
- Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. 2002;347:408–415. - PubMed
-
- Walsh TJ, Anaissie EJ, Denning DW, et al. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:327–360. - PubMed
-
- Hope WW, Walsh TJ, Denning DW. Laboratory diagnosis of invasive aspergillosis. Lancet Infect Dis. 2005;5:609–622. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources