

The contribution of risk factors to socioeconomic inequalities in multimorbidity across the lifecourse: a longitudinal analysis of the Twenty-07 cohort
- PMID: 28835246
- PMCID: PMC5569487
- DOI: 10.1186/s12916-017-0913-6
The contribution of risk factors to socioeconomic inequalities in multimorbidity across the lifecourse: a longitudinal analysis of the Twenty-07 cohort
Abstract
Background: Multimorbidity is a major challenge to health systems globally and disproportionately affects socioeconomically disadvantaged populations. We examined socioeconomic inequalities in developing multimorbidity across the lifecourse and investigated the contribution of five behaviour-related risk factors.
Methods: The Twenty-07 study recruited participants aged approximately 15, 35, and 55 years in 1987 and followed them up over 20 years. The primary outcome was development of multimorbidity (2+ health conditions). The relationship between five different risk factors (smoking, alcohol consumption, diet, body mass index (BMI), physical activity) and the development of multimorbidity was assessed. Social patterning in the development of multimorbidity based on two measures of socioeconomic status (area-based deprivation and household income) was then determined, followed by investigation of potential mediation by the five risk factors. Multilevel logistic regression models and predictive margins were used for statistical analyses. Socioeconomic inequalities in multimorbidity were quantified using relative indices of inequality and attenuation assessed through addition of risk factors.
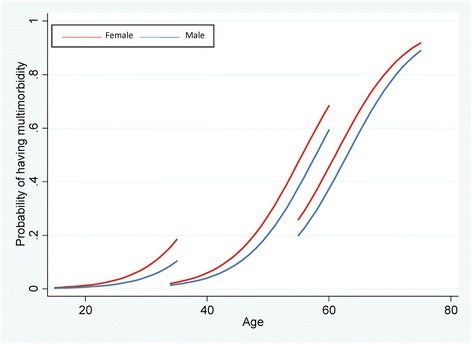
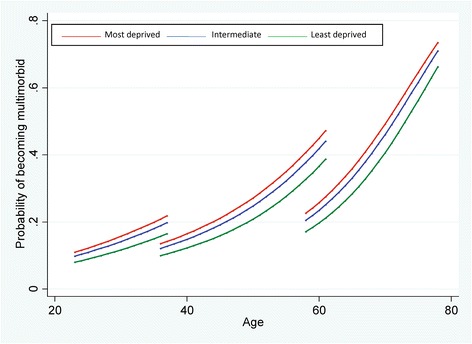
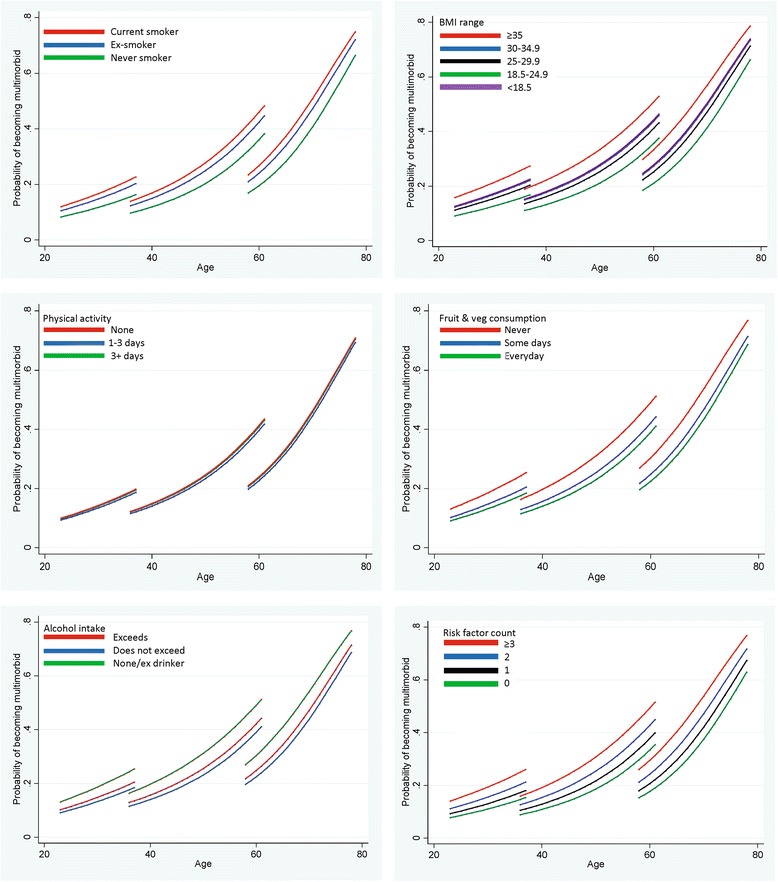
Results: Multimorbidity prevalence increased markedly in all cohorts over the 20 years. Socioeconomic disadvantage was associated with increased risk of developing multimorbidity (most vs least deprived areas: odds ratio (OR) 1.46, 95% confidence interval (CI) 1.26-1.68), and the risk was at least as great when assessed by income (OR 1.53, 95% CI 1.25-1.87) or when defining multimorbidity as 3+ conditions. Smoking (current vs never OR 1.56, 1.36-1.78), diet (no fruit/vegetable consumption in previous week vs consumption every day OR 1.57, 95% CI 1.33-1.84), and BMI (morbidly obese vs healthy weight OR 1.88, 95% CI 1.42-2.49) were strong independent predictors of developing multimorbidity. A dose-response relationship was observed with number of risk factors and subsequent multimorbidity (3+ risk factors vs none OR 1.91, 95% CI 1.57-2.33). However, the five risk factors combined explained only 40.8% of socioeconomic inequalities in multimorbidity development.
Conclusions: Preventive measures addressing known risk factors, particularly obesity and smoking, could reduce the future multimorbidity burden. However, major socioeconomic inequalities in the development of multimorbidity exist even after taking account of known risk factors. Tackling social determinants of health, including holistic health and social care, is necessary if the rising burden of multimorbidity in disadvantaged populations is to be redressed.
Keywords: Comorbidity; Health behaviour; Health care disparities; Multimorbidity; Risk factors; Socioeconomic status.
Conflict of interest statement
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
