

Positional Skull Deformities
- PMID: 28835328
- PMCID: PMC5624275
- DOI: 10.3238/arztebl.2017.0535
Positional Skull Deformities
Abstract
Background: Especially in the first 6 months of life, skull deformities manifesting as a uni- or bilateral flattening of the occiput often give rise to questions of differential diagnosis and potential treatment. In this review, the authors summarize the current understanding of risk factors for this condition, and the current state of the relevant diagnostic assessment and options for treatment.
Methods: The recommendations given in this selective review of the literature are based on current studies and on existing guidelines on the prevention of sudden infant death, the recommendations of the German Society for Pediatric Neurology (Deutsche Gesellschaft für Neuropädiatrie), and the American guidelines on the treatment of positional plagiocephaly in infancy.
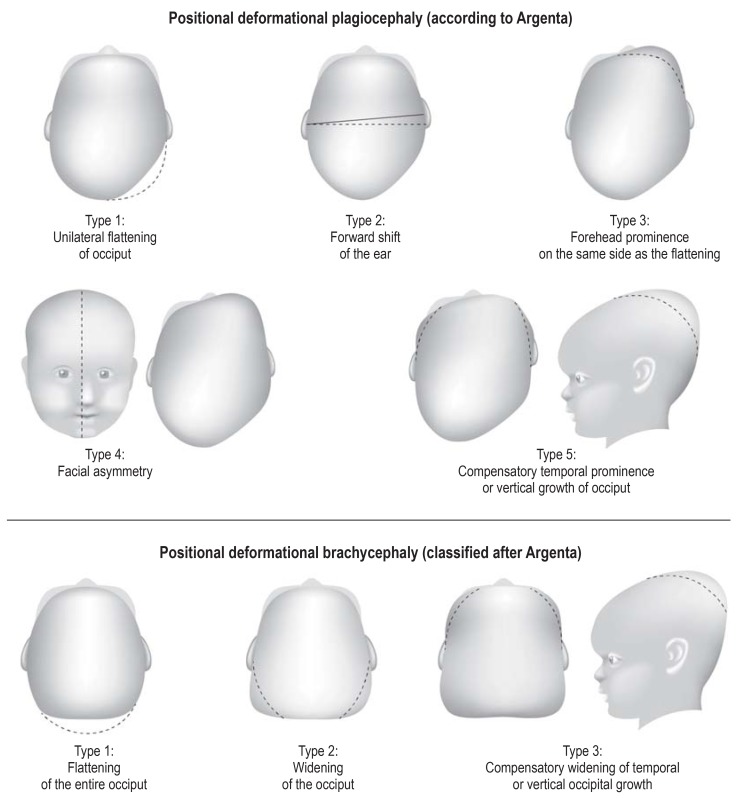
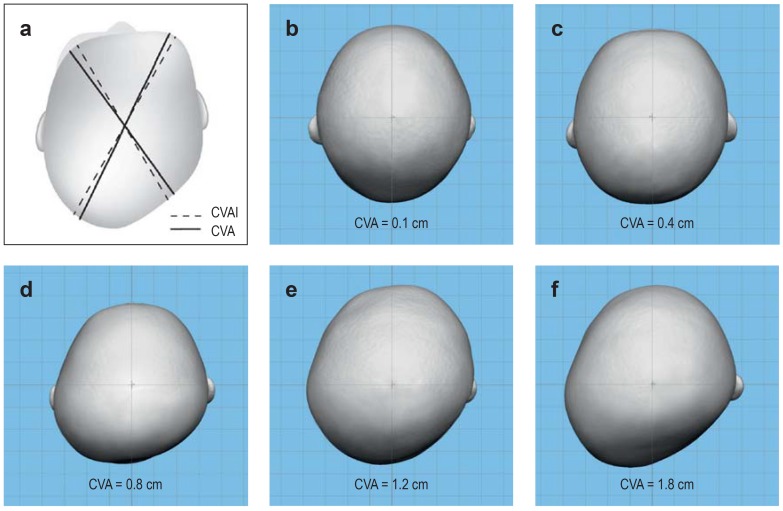
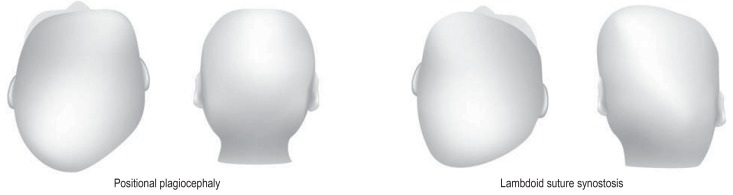
Results: Pre-, peri-, and postnatal risk factors can contribute to the development of positional skull deformities. These deformities can be diagnosed and classified on the basis of their clinical features, supplemented in unclear cases by ultrasonography of the cranial sutures. The putative relationship between positional skull deformities and developmental delay is currently debated. The main preventive and therapeutic measure is parent education to foster correct positioning habits (turning of the infant to the less favored side; prone positioning on occasion when awake) and beneficial stimulation of the infant (to promote lying on the less favored side). If the range of motion of the head is limited, physiotherapy is an effective additional measure. In severe or refractory cases, a skull orthosis (splint) may be useful.
Conclusion: The parents of children with positional skull deformities should be comprehensively informed about the necessary preventive and therapeutic measures. Treatment should be initiated early and provided in graded fashion, according to the degree of severity of the problem. Parental concern about the deformity should not be allowed to lead to a rejection of the reasonable recommendation for a supine sleeping position.
Figures


Comment in
-
The Cause is Cesarean Section.Dtsch Arztebl Int. 2018 Jan 19;115(3):38. doi: 10.3238/arztebl.2018.0038b. Dtsch Arztebl Int. 2018. PMID: 29366452 Free PMC article. No abstract available.
-
Osteopathy as an Aid to Treatment.Dtsch Arztebl Int. 2018 Jan 19;115(3):38-39. doi: 10.3238/arztebl.2018.0038c. Dtsch Arztebl Int. 2018. PMID: 29366453 Free PMC article. No abstract available.
-
Caused by Spinal Block.Dtsch Arztebl Int. 2018 Jan 19;115(3):39. doi: 10.3238/arztebl.2018.0039a. Dtsch Arztebl Int. 2018. PMID: 29366454 Free PMC article. No abstract available.
References
-
- American Academy of Pediatrics. AAP Task Force on Infant Positioning and SIDS: positioning and SIDS. Pediatrics. 1992;89:1120–1126. - PubMed
-
- Arbeitsgemeinschaft der Wissenschaftlichen. Medizinischen Fachgesellschaften, Leitlinie der Deutschen Gesellschaft für Schlafmedizin Nr. 063/002, S1-Leitlinie. Plötzlicher Säuglingstod. 01/2012.
-
- AAP Task Force on sudden infant death syndrome. SIDS and other sleep-related infant deaths: updated 2016 recommendations for a safe infant sleeping environment. Pediatrics. 2016;138 e20162938. - PubMed
-
- Flannery AM, Tamber MS, Mazzola C, et al. Congress of neurological surgeons systematic review and evidence-based guidelines for the management of patients with positional plagiocephaly: executive summary. Neurosurgery. 2016;79:623–624. - PubMed
-
- Rosenbaum T, Borusiak P, Schweitzer T, et al. Dynamische Kopforthesen („Helmtherapie“) Stellungnahme der gemeinsamen Therapiekommission der Gesellschaft für Neuropädiatrie und der Deutschen Gesellschaft für Sozialpädiatrie und Jugendmedizin 2012. Neuropädiatrie in Klinik und Praxis. 2014;1:4–9.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources