

Vitamin D prenatal programming of childhood metabolomics profiles at age 3 y
- PMID: 28835366
- PMCID: PMC5611786
- DOI: 10.3945/ajcn.117.158220
Vitamin D prenatal programming of childhood metabolomics profiles at age 3 y
Abstract
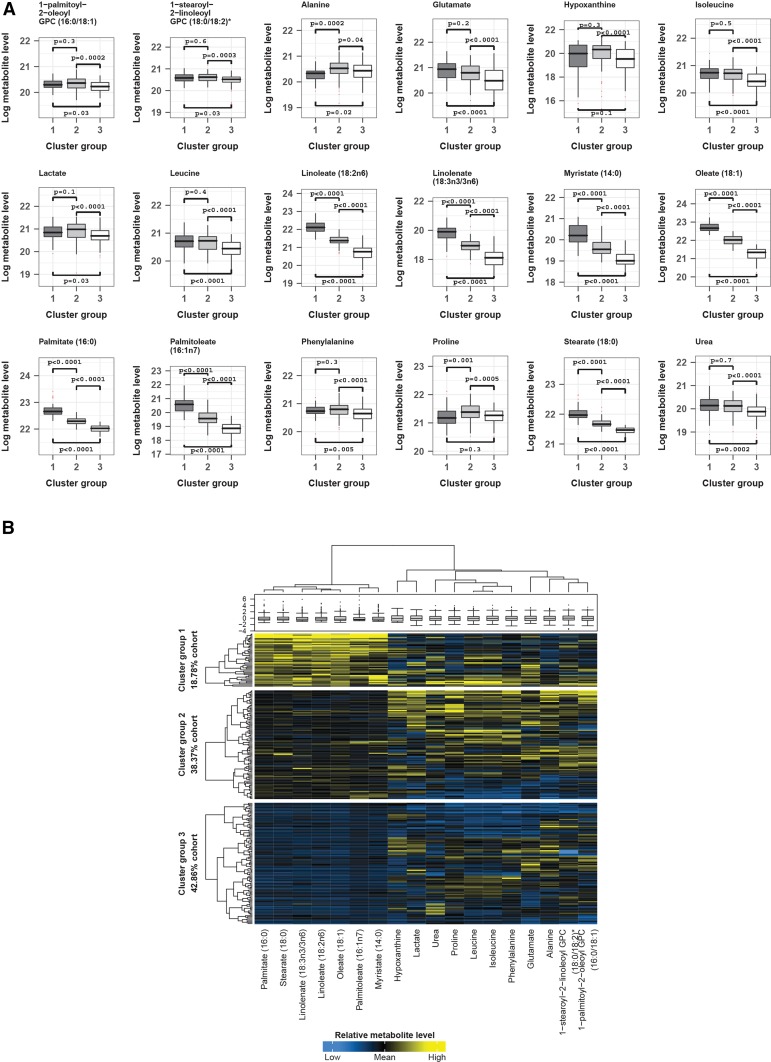
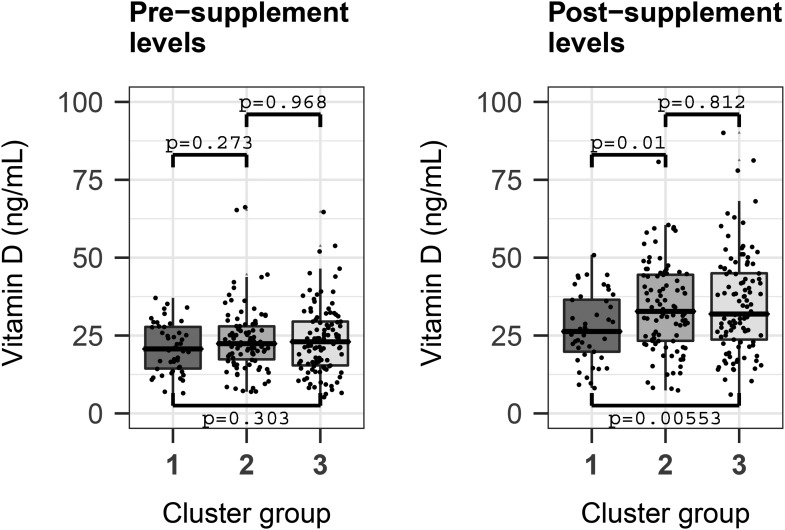
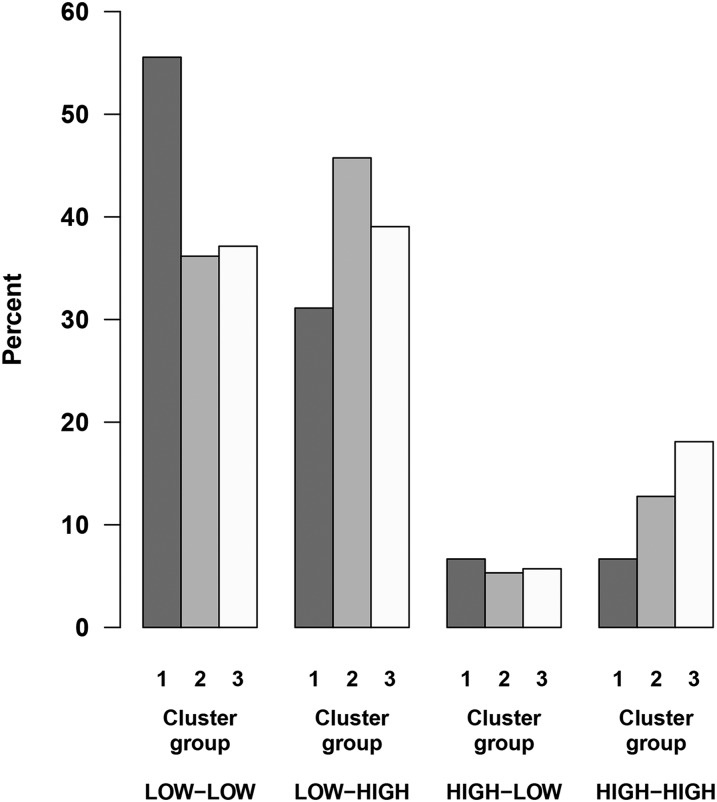
Background: Vitamin D deficiency is implicated in a range of common complex diseases that may be prevented by gestational vitamin D repletion. Understanding the metabolic mechanisms related to in utero vitamin D exposure may therefore shed light on complex disease susceptibility.Objective: The goal was to analyze the programming role of in utero vitamin D exposure on children's metabolomics profiles.Design: First, unsupervised clustering was done with plasma metabolomics profiles from a case-control subset of 245 children aged 3 y with and without asthma from the Vitamin D Antenatal Asthma Reduction Trial (VDAART), in which pregnant women were randomly assigned to vitamin D supplementation or placebo. Thereafter, we analyzed the influence of maternal pre- and postsupplement vitamin D concentrations on cluster membership. Finally, we used the metabolites driving the clustering of children to identify the dominant metabolic pathways that were influential in each cluster.Results: We identified 3 clusters of children characterized by 1) high concentrations of fatty acids and amines and low maternal postsupplement vitamin D (mean ± SD; 27.5 ± 11.0 ng/mL), 2) high concentrations of amines, moderate concentrations of fatty acids, and normal maternal postsupplement vitamin D (34.0 ± 14.1 ng/mL), and 3) low concentrations of fatty acids, amines, and normal maternal postsupplement vitamin D (35.2 ± 15.9 ng/mL). Adjusting for sample storage time, maternal age and education, and both child asthma and vitamin D concentration at age 3 y did not modify the association between maternal postsupplement vitamin D and cluster membership (P = 0.0014). Maternal presupplement vitamin D did not influence cluster membership, whereas the combination of pre- and postsupplement concentrations did (P = 0.03).Conclusions: Young children can be clustered into distinct biologically meaningful groups by their metabolomics profiles. The clusters differed in concentrations of inflammatory mediators, and cluster membership was influenced by in utero vitamin D exposure, suggesting a prenatal programming role of vitamin D on the child's metabolome. This trial was registered at clinicaltrials.gov as NCT00920621.
Keywords: airway inflammation; metabolomics; polyunsaturated fatty acids; prenatal programming; vitamin D.
© 2017 American Society for Nutrition.
Figures
References
-
- Müller MJ, Volmer DA. Mass spectrometric profiling of vitamin D metabolites beyond 25-hydroxyvitamin D. Clin Chem 2015;61:1033–48. - PubMed
-
- Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266–81. - PubMed
-
- Ginde AA, Mansbach JM, Camargo CA. Vitamin D, respiratory infections, and asthma. Curr Allergy Asthma Rep 2009;9:81–7. - PubMed
-
- Pilz S, Verheyen N, Grubler MR, Tomaschitz A, Marz W. Vitamin D and cardiovascular disease prevention. Nat Rev Cardiol 2016;13:404–17. - PubMed
-
- Deeb KK, Trump DL, Johnson CS. Vitamin D signalling pathways in cancer: potential for anticancer therapeutics. Nat Rev Cancer 2007;7:684–700. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
