

Review
doi: 10.1038/nrc.2017.60.
Therapy-related myeloid neoplasms: when genetics and environment collide
Affiliations
- PMID: 28835720
- PMCID: PMC5946699
- DOI: 10.1038/nrc.2017.60
Item in Clipboard
Review
Therapy-related myeloid neoplasms: when genetics and environment collide
Nat Rev Cancer.
.
Abstract
Therapy-related myeloid neoplasms (t-MN) arise as a late effect of chemotherapy and/or radiation administered for a primary condition, typically a malignant disease, solid organ transplant or autoimmune disease. Survival is measured in months, not years, making t-MN one of the most aggressive and lethal cancers. In this Review, we discuss recent developments that reframe our understanding of the genetic and environmental aetiology of t-MN. Emerging data are illuminating who is at highest risk of developing t-MN, why t-MN are chemoresistant and how we may use this information to treat and ultimately prevent this lethal disease.
Conflict of interest statement
Figures
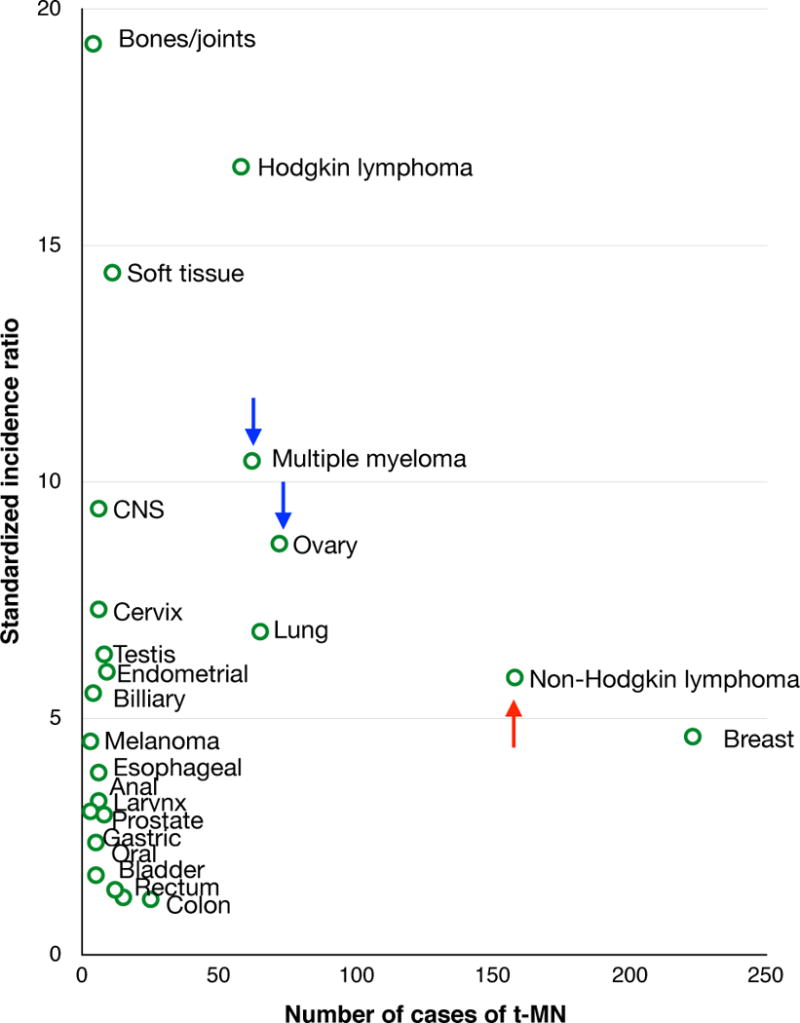
Among adults treated with chemotherapy for a primary malignancy, 801 t-MN patients were identified from Surveillance, Epidemiology and End Results. The number of cases and standardized incidence ratio for t-MN are shown by primary tumor type. The risk of t-MN has decreased over time for patients with multiple myeloma or ovarian cancer (blue arrows), whereas the risk has increased for patients with non-Hodgkin lymphoma (red arrow).
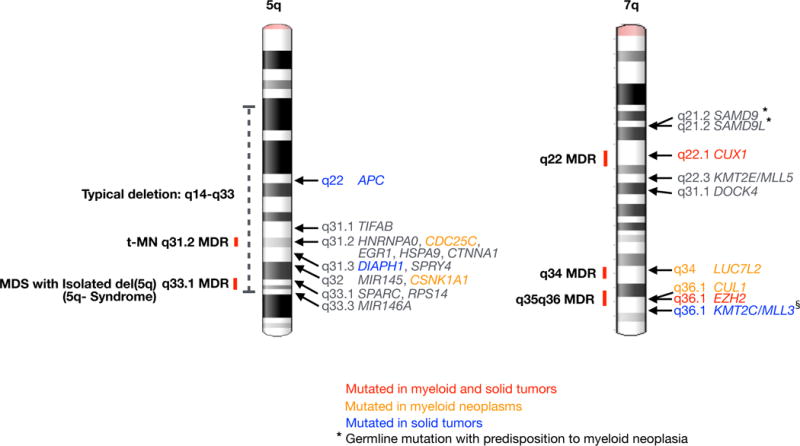
Minimally deleted regions (MDRs) on the long arms of chromosomes 5, and 7– are shown. In t-MN, there is evidence for a role for haploinsufficiency of the following genes on 5q: APC, TIFAB, and EGR1. HNRNPA0, HSPA9, DIAPH1, and SPRY4 have been implicated based on mouse models, and mutations of CDC25C have been identified in FPD/AML (familial platelet disorder progressing to AML). CTNNA1 has been implicated in some, but not all, studies. MIR145, MIR146A, CSNK1A1, SPARC, and RPS14 have been shown to be involved in the pathogenesis of MDS with an Isolated del(5q). On 7q, there is evidence for a role in myeloid neoplasia for these genes: SAMD9, SAMD9L,, CUX1, KMT2E–, DOCK4
LUC7L2, CUL1, EZH2, and KMT2C. Blue text indicates genes significantly, recurrently mutated in pan-cancer analysis. Orange text indicates genes recurrently mutated in myeloid neoplasms. Red text indicates genes recurrently mutated in both myeloid and pan-cancer. §
KMT2C/MLL3 mutations may be overestimated due to a pseudogene causing false positive mutations. * Genes with inherited mutations that are associated with a predisposition to myeloid dysplasia are indicated.
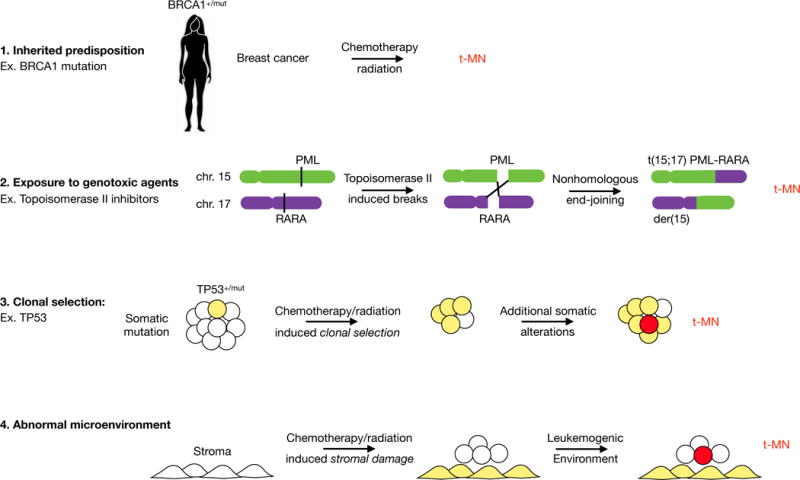
There are four main drivers for therapy-related myeloid neoplasia development. These pathways are not mutually exclusive, and one or multiple pathways may contribute in any individual patient. 1. Patients with an inherited mutation in a gene encoding a component of the DNA damage and repair response pathway have an increased susceptibility to the development of multiple, independent malignancies. In addition, these patients may have increased susceptibility to chemotherapy/radiation-induced mutations due to an impaired DNA damage response or DNA repair pathway. 2. The role for therapy as a mutagen is illustrated. In the prevailing model of t-MN, chemotherapy/radiation induces DNA damage that leads to transformation. An example of this is topoisomerase-II inhibitor induced translocations. 3. The role for therapy as a driver of clonal selection is shown. In patients with a pre-existing somatic mutation and clonal hematopoiesis, i.e., clonal hematopoiesis of indeterminate potential, chemotherapy/radiation gives these clones a competitive advantage over normal HSCs. The consequences of the somatic mutation – genetic instability associated with mutant TP53, for example – combined with regenerative hematopoiesis facilitates the acquisition of subsequent mutations and t-MN development. 4. Chemotherapy/radiation also induces damage to the bone marrow stromal niche. Alternatively, the bone marrow microenvironment may be altered/damaged due to normal processes, e.g., aging. Altered niche function, such as pro-inflammatory response, may promote clonal selection and/or produce factors that favor leukemia initiating cells.
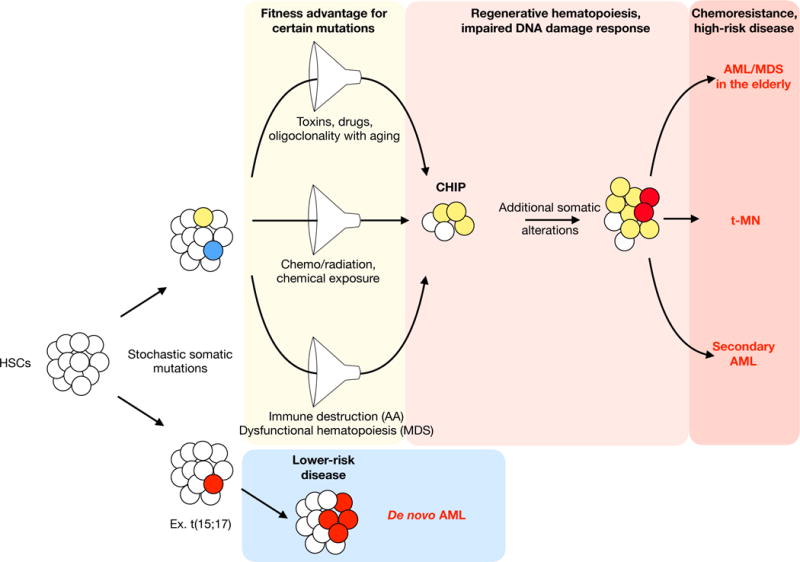
Stochastic mutations occur in hematopoietic stem cells over time. Certain mutated genes provide a “fitness” advantage in the context of various competitive conditions. Competition filters for mutant HSCs at the expense of healthy HSCs, resulting in clonal hematopoiesis of indeterminate potential (CHIP). Over time, mutant clones can acquire additional mutations due to mutations in the DNA damage response genes and/or increased proliferation in the context of regenerative hematopoiesis. In hematopoiesis, competition arises in a number of different contexts. Loss of HSC diversity with age, and the cumulative lifetime exposure to toxins and drugs, among other factors, may select for mutant clones that ultimately give rise to myeloid neoplasms in the elderly. Chemotherapy and radiation exposure promotes therapy-related myeloid neoplasms. Inflammation, immune destruction, and dysfunctional hematopoiesis (including niche-based effects) can give rise to secondary myeloid neoplasms arising from aplastic anemia or myelodysplastic syndrome. Regardless of the selective pressure, the competitive filter increases the likelihood that the malignant clones will have inherent therapy resistance. In contrast, a stochastic mutation that gives rise to AML without an antecedent clonal selection is more likely to be lower-risk disease.

A proportion of t-MN derives from clonal selection of hematopoietic stem cells (HSCs) carrying somatic mutations (indicated by an “M” in the illustration) at the expense of healthy HSCs during treatment of the primary cancer. One hypothetical approach towards preserving the healthy HSCs is to temporarily recapitulate the mutation in the healthy HSCs, such that no HSC clone has a “fitness” advantage over the others. For example, in patients with a somatic TP53 mutation, a TP53 inhibitor administered during chemotherapy/radiation treatment would prevent normal HSCs from being out-competed by TP53-mutant HSCs. A similar strategy could be devised for other CHIP mutations.
References
-
- Singh ZN, et al. Therapy-related myelodysplastic syndrome: morphologic subclassification may not be clinically relevant. American Journal of Clinical Patholology. 2007;127:197–205. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
