

Relapsing/remitting type 1 diabetes
- PMID: 28835984
- PMCID: PMC6448902
- DOI: 10.1007/s00125-017-4403-3
Relapsing/remitting type 1 diabetes
Abstract
Aims/hypothesis: Type 1 diabetes is believed to be an autoimmune disease associated with irreversible loss of insulin secretory function that follows a chronic progressive course. However, it has been speculated that relapsing/remitting disease progression may occur in type 1 diabetes.
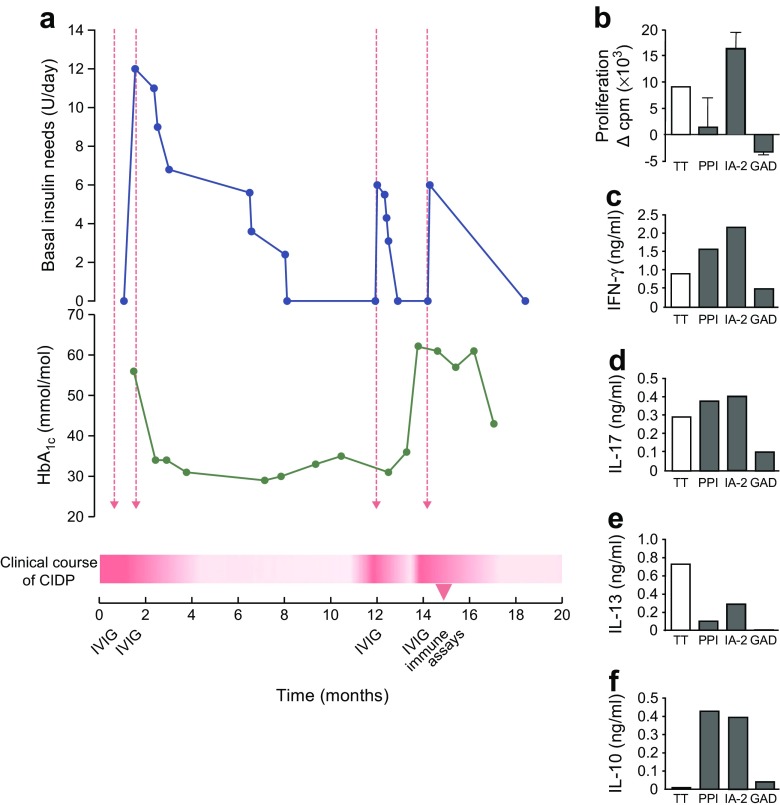
Methods: We report the case of an 18-year-old girl with Graves' disease, chronic inflammatory demyelinating polyneuropathy (CIDP) and multiple islet autoantibodies, presenting with relapsing/remitting hyperglycaemia. Peripheral blood mononuclear cells were analysed for islet autoimmunity.
Results: There were two instances of hyperglycaemia relapse during CIDP flare-ups that required insulin therapy and remitted after i.v. immunoglobulin (IVIG) therapy improving neurological symptoms. A diagnosis of type 1 diabetes was assigned on the basis of insulin need, HbA1c and islet autoantibodies. Insulin requirements disappeared following IVIG treatment and peaked during CIDP flare-ups. Pro- and anti-inflammatory cytokine responses were noted against islet autoantigens.
Conclusions/interpretation: We provide clinical evidence of relapsing/remitting type 1 diabetes associated with IVIG treatment and the regulation of islet autoimmunity. Despite sufficient residual beta cell mass, individuals can experience episodes of impaired glycaemia control. This disconnect between beta cell mass and function highlighted by our case may have implications for the use of beta cell function as the primary endpoint for immune intervention trials aiming to protect beta cell mass rather than function. Immune modulation may restore beta cell function and glycaemic control.
Keywords: Autoimmune disease; Immune regulation; Immunotherapy; Type 1 diabetes.
Conflict of interest statement
Data availability
The datasets collected in this study are available from the corresponding author on request.
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
MPS, FMK and KMM contributed equally: they performed the immunological experiments, analysed and researched data, and wrote the manuscript. TN and BR analysed the data, reviewed/edited the manuscript and contributed to the discussion. IB, FS and AR-K contributed to conception and design of this report, acquired data and revised the manuscript. All authors gave final approval of the version to be published. BR is responsible for the integrity of the work as a whole.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
