

Laparoscopic ultrasonography as an alternative to intraoperative cholangiography during laparoscopic cholecystectomy
- PMID: 28839445
- PMCID: PMC5550794
- DOI: 10.3748/wjg.v23.i29.5438
Laparoscopic ultrasonography as an alternative to intraoperative cholangiography during laparoscopic cholecystectomy
Abstract
Aim: To assess the role of laparoscopic ultrasound (LUS) as a substitute for intraoperative cholangiography (IOC) during cholecystectomy.
Methods: We present a MEDLINE and PubMed literature search, having used the key-words "laparoscopic intraoperative ultrasound" and "laparoscopic cholecystectomy". All relevant English language publications from 2000 to 2016 were identified, with data extracted for the role of LUS in the anatomical delineation of the biliary tract, detection of common bile duct stones (CBDS), prevention or early detection of biliary duct injury (BDI), and incidental findings during laparoscopic cholecystectomy. Data for the role of LUS vs IOC in complex situations (i.e., inflammatory disease/fibrosis) were specifically analyzed.
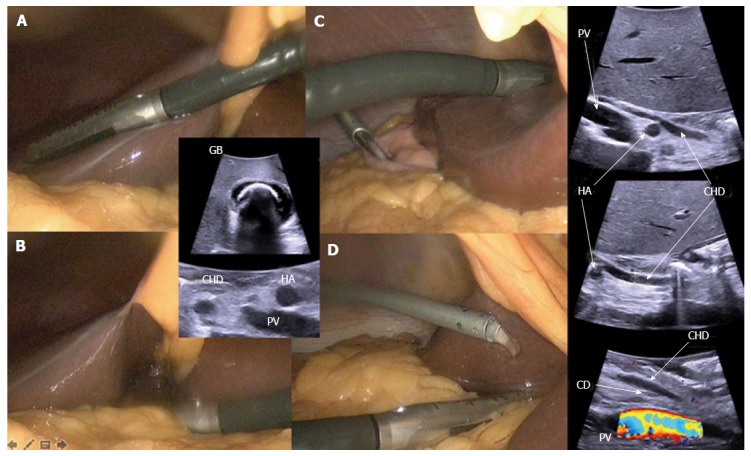
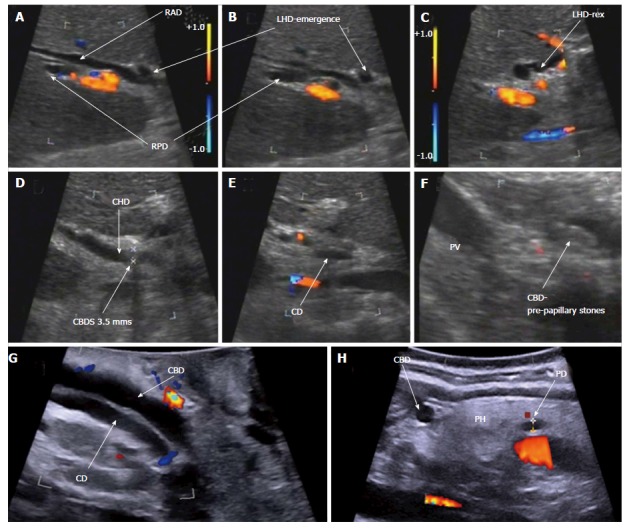
Results: We report data from eighteen reports, 13 prospective non-randomized trials, 5 retrospective trials, and two meta-analyses assessing diagnostic accuracy, with one analysis also assessing costs, duration of the examination, and anatomical mapping. Overall, LUS was shown to provide highly sensitive mapping of the extra-pancreatic biliary anatomy in 92%-100% of patients, with more difficulty encountered in delineation of the intra-pancreatic segment of the biliary tract (73.8%-98%). Identification of vascular and biliary variations has been documented in two studies. Although inflammatory disease hampered accuracy, LUS was still advantageous vs IOC in patients with obscured anatomy. LUS can be performed before any dissection and repeated at will to guide the surgeon especially when hilar mapping is difficult due to fibrosis and inflammation. In two studies LUS prevented conversion in 91% of patients with difficult scenarios. Considering CBDS detection, LUS sensitivity and specificity were 76%-100% and 96.2%-100%, respectively. LUS allowed the diagnosis/treatment of incidental findings of adjacent organs. No valuable data for BDI prevention or detection could be retrieved, even if no BDI was documented in the reports analyzed. Literature analysis proved LUS as a safe, quick, non-irradiating, cost-effective technique, which is comparatively well known although largely under-utilized, probably due to the perception of a difficult learning curve.
Conclusion: We highlight the advantages and limitations of laparoscopic ultrasound during cholecystectomy, and underline its value in difficult scenarios when the anatomy is obscured.
Keywords: Bile duct injury; Biliary anomalies; Choledocolithiasis; Intraoperative ultrasound; Laparoscopic cholecystectomy.
Conflict of interest statement
Conflict-of-interest statement: No potential conflicts of interest.
Figures
References
-
- Gallstones and laparoscopic cholecystectomy. NIH Consensus Development Panel on Gallstones and Laparoscopic Cholecystectomy. Surg Endosc. 1993;7:271–279. - PubMed
-
- Hogan NM, Dorcaratto D, Hogan AM, Nasirawan F, McEntee P, Maguire D, Geoghegan J, Traynor O, Winter DC, Hoti E. Iatrogenic common bile duct injuries: Increasing complexity in the laparoscopic era: A prospective cohort study. Int J Surg. 2016;33 Pt A:151–156. - PubMed
-
- Halbert C, Pagkratis S, Yang J, Meng Z, Altieri MS, Parikh P, Pryor A, Talamini M, Telem DA. Beyond the learning curve: incidence of bile duct injuries following laparoscopic cholecystectomy normalize to open in the modern era. Surg Endosc. 2016;30:2239–2243. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
