

Transnasal endoscopy: no gagging no panic!
- PMID: 28839865
- PMCID: PMC5369487
- DOI: 10.1136/flgastro-2015-100589
Transnasal endoscopy: no gagging no panic!
Abstract
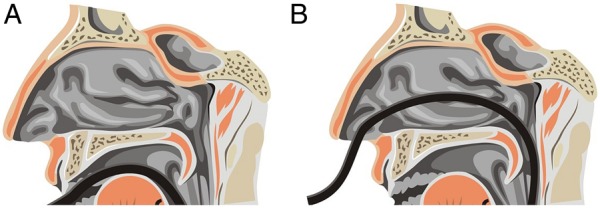
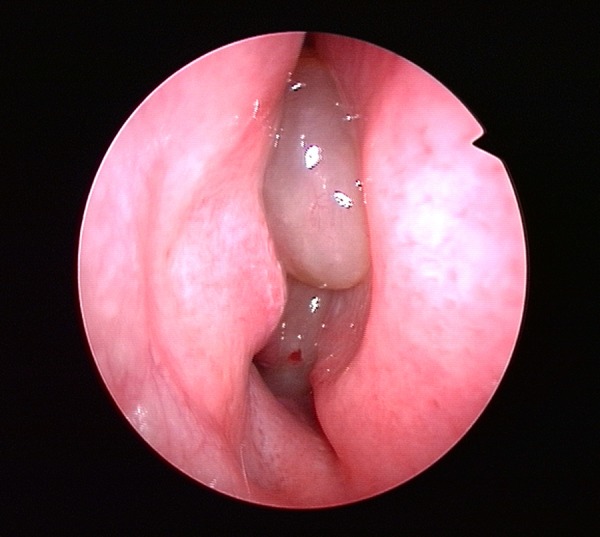
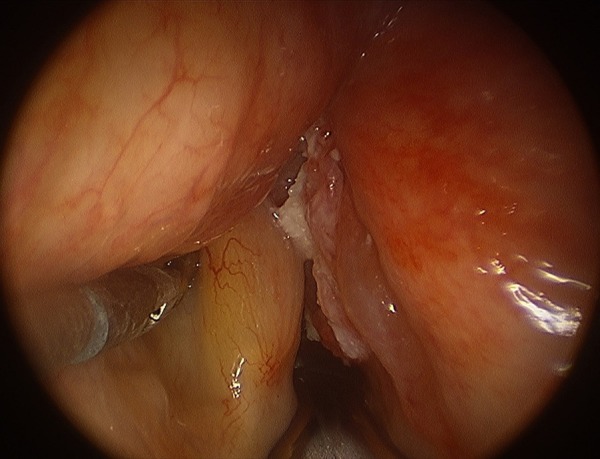
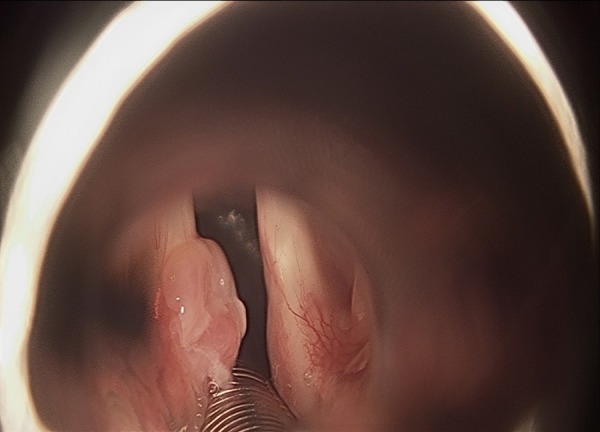
Background: Transnasal endoscopy (TNE) is performed with an ultrathin scope via the nasal passages and is increasingly used. This review covers the technical characteristics, tolerability, safety and acceptability of TNE and also diagnostic accuracy, use as a screening tool and therapeutic applications. It includes practical advice from an ear, nose, throat (ENT) specialist to optimise TNE practice, identify ENT pathology and manage complications.
Methods: A Medline search was performed using the terms "transnasal", "ultrathin", "small calibre", "endoscopy", "EGD" to identify relevant literature.
Results: There is increasing evidence that TNE is better tolerated than standard endoscopy as measured using visual analogue scales, and the main area of discomfort is nasal during insertion of the TN endoscope, which seems remediable with adequate topical anaesthesia. The diagnostic yield has been found to be similar for detection of Barrett's oesophagus, gastric cancer and GORD-associated diseases. There are some potential issues regarding the accuracy of TNE in detecting small early gastric malignant lesions, especially those in the proximal stomach. TNE is feasible and safe in a primary care population and is ideal for screening for upper gastrointestinal pathology. It has an advantage as a diagnostic tool in the elderly and those with multiple comorbidities due to fewer adverse effects on the cardiovascular system. It has significant advantages for therapeutic procedures, especially negotiating upper oesophageal strictures and insertion of nasoenteric feeding tubes.
Conclusions: TNE is well tolerated and a valuable diagnostic tool. Further evidence is required to establish its accuracy for the diagnosis of early and small gastric malignancies. There is an emerging role for TNE in therapeutic endoscopy, which needs further study.
Keywords: BARRETT'S OESOPHAGUS; DIAGNOSTIC AND THERAPEUTIC ENDOSCOPY; ENDOSCOPY; GASTRIC CANCER; OESOPHAGEAL VARICES.
Figures
References
-
- Quine MA, Bell GD, McCloy RF, et al. . Prospective audit of upper gastrointestinal endoscopy in two regions of England: safety, staffing and sedation methods. Gut 1995;36:462–7. doi:10.1136/gut.36.3.462 - DOI - PMC - PubMed
-
- Sharma VK, Nguyen CC, Crowell MD. A national study of cardiopulmonary unplanned events after GI endoscopy. Gastrointest Endosc 2007;66:27–34. doi:10.1016/j.gie.2006.12.040 - DOI - PubMed
-
- Mori A, Ohashi N, Tatebe H. Autonomic nervous function in upper GI endoscopy: a prospective randomised comparison between transnasal and oral procedures. J Gastroenterol 2008;43:38–44. doi:10.1007/s00535-007-2124-y - DOI - PubMed
-
- Garcia RT, Cello JP, Nguyen MH. Unsedated ultrathin EGD is well accepted when compared with conventional sedated EGD: a multicentre randomised trial. Gastroenterology 2003;125:1606–12. doi:10.1053/j.gastro.2003.08.034 - DOI - PubMed
-
- Jobe BA, Hunter JG, Chang EY. Office-based unsedated small caliber endoscopy is equivalent to conventional sedated endoscopy in screening and sureveillance for Barretts esophagus: a randomised and blinded comparison. Am J Gastroenterol 2006;101:2693–703. doi:10.1111/j.1572-0241.2006.00890.x - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous