

The impact of alteplase on pulmonary graft function in donation after circulatory death - An experimental study
- PMID: 28839932
- PMCID: PMC5560118
- DOI: 10.1016/j.amsu.2017.08.010
The impact of alteplase on pulmonary graft function in donation after circulatory death - An experimental study
Abstract
Objective: Lung transplantation is hampered by the lack of organs resulting in deaths on the waiting list. The usage of donation after circulatory death (DCD) lungs would dramatically increase donor availability. The most optimal organ preservation method, and the need for antithrombotic and fibrinolytic treatment to prevent thrombosis in the donor lungs is currently on debate. The present study investigated, in a simulated clinical DCD situation, whether the addition of alteplase in the flush-perfusion solution at the time of pulmonary graft harvesting could prevent thrombosis in the donor lung and thereby improve pulmonary graft function.
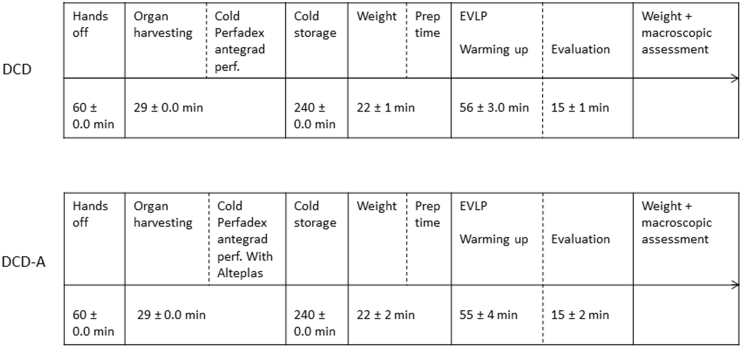
Methods: Twelve Swedish domestic pigs were randomized into two groups. All animals underwent ventricular fibrillation and were then left untouched for 1 h after declaration of death. None of the animals received heparin. The lungs were then harvested and flush-perfused with Perfadex® solution and the organs were then stored at 8 °C for 4 h. In one group alteplase was added to the Perfadex® solution (donation after cardiac death with alteplase (DCD-A)) and in the other, it was not (DCD). Lung function was evaluated, using ex vivo lung perfusion (EVLP), with blood gases at different oxygen levels, pulmonary vascular resistance (PVR), lung weight, and macroscopic appearance.
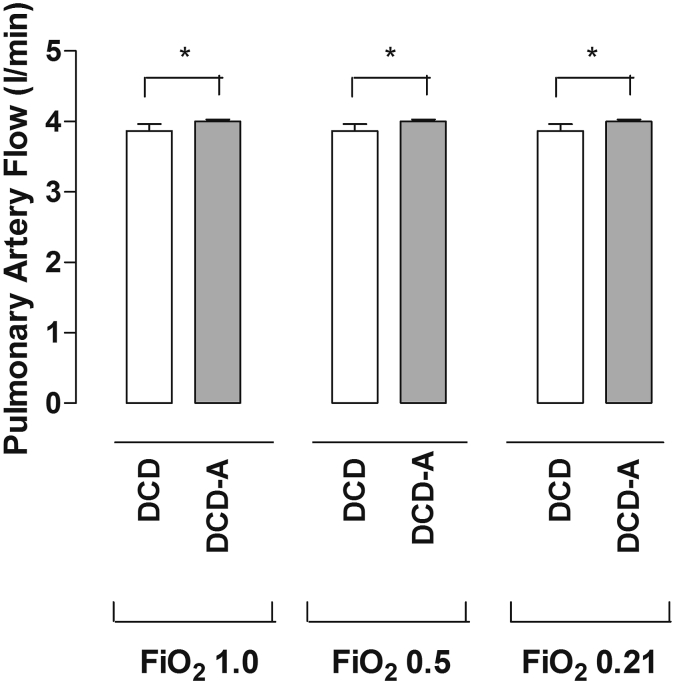
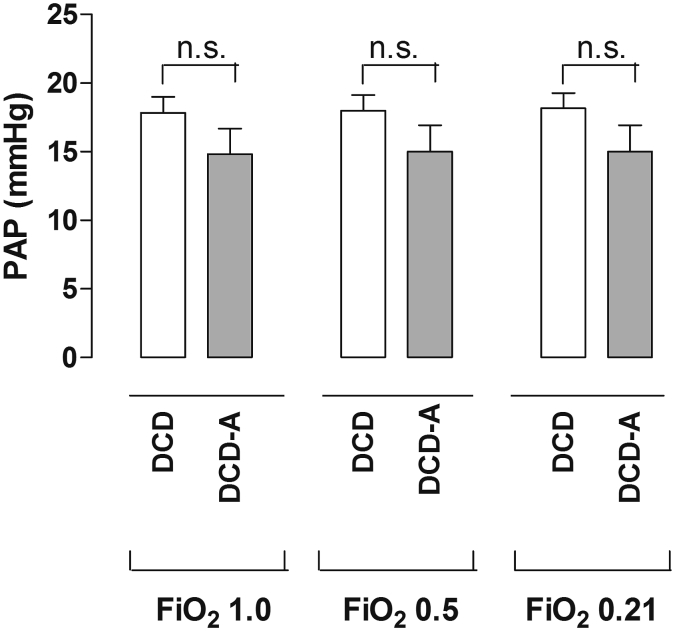
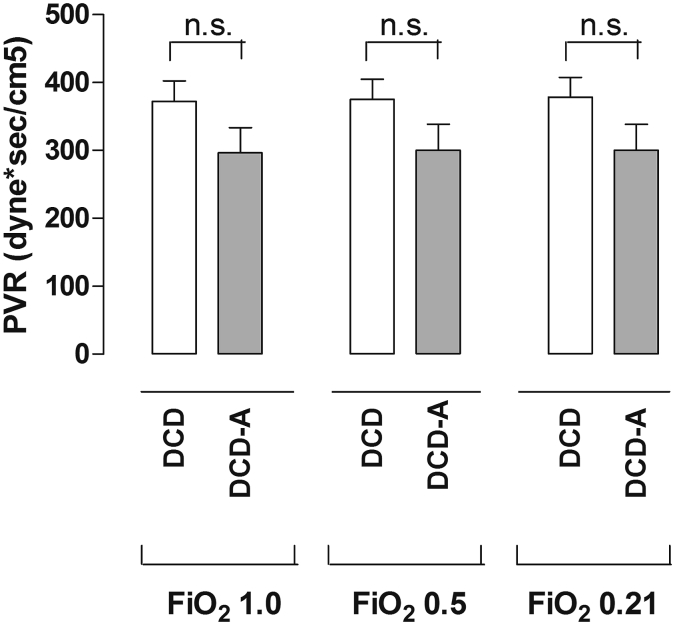
Results: During EVLP, there were no significant differences between groups in PaO2 at any investigated FiO2 level (1.0, 0.5, or 0.21). At FiO2 1.0, the PaO2 in the DCD and DCD-A was 51.7 ± 2.05 kPa and 60.3 ± 3.67 kPa, respectively (p = 0.1320). There were no significant differences between groups PVR levels, in the DCD (372 ± 31 dyne x s/cm5) and in the DCD-A (297 ± 37 dyne x s/cm5) groups (p = 0.1720). There was no significant difference between groups in macroscopic appearance.
Conclusions: All the lungs showed excellent blood gases after EVLP, and they all meet the criteria's for clinical lung transplantation. The use of alteplase did not seem to have any obvious benefit to the donor lungs in a DCD situation. The donor lungs treated with alteplas showed slightly better blood gases and slightly lower PVR compared to the group without alteplas, however the difference was not significant. DCD appears to be a safe and effective method to expand the donor pool.
Keywords: DCD; EVLP; Lung transplantation; Pulmonary graft.
Figures
Similar articles
-
Lungs exposed to 1 hour warm ischemia without heparin before harvesting might be suitable candidates for transplantation.J Cardiothorac Surg. 2015 Oct 23;10:131. doi: 10.1186/s13019-015-0339-1. J Cardiothorac Surg. 2015. PMID: 26500001 Free PMC article.
-
Heparin does not improve graft function in uncontrolled non-heart-beating lung donation: an experimental study in pigs.Eur J Cardiothorac Surg. 2013 Feb;43(2):413-9. doi: 10.1093/ejcts/ezs364. Epub 2012 Jul 3. Eur J Cardiothorac Surg. 2013. PMID: 22761497
-
Ex vivo MFG-E8 treatment improves the function of lungs procured from cardiac death donors in preclinical porcine model.Heliyon. 2024 Jun 25;10(13):e33614. doi: 10.1016/j.heliyon.2024.e33614. eCollection 2024 Jul 15. Heliyon. 2024. PMID: 39040292 Free PMC article.
-
Strategies for safe donor expansion: donor management, donations after cardiac death, ex-vivo lung perfusion.Curr Opin Organ Transplant. 2013 Oct;18(5):513-7. doi: 10.1097/MOT.0b013e328365191b. Curr Opin Organ Transplant. 2013. PMID: 23995370 Review.
-
Expanding the lung donor pool: advancements and emerging pathways.Curr Opin Organ Transplant. 2015 Oct;20(5):498-505. doi: 10.1097/MOT.0000000000000233. Curr Opin Organ Transplant. 2015. PMID: 26262464 Review.
Cited by
-
Ischemia-Reperfusion Injury in Lung Transplantation.Cells. 2021 May 28;10(6):1333. doi: 10.3390/cells10061333. Cells. 2021. PMID: 34071255 Free PMC article. Review.
-
Perfusion fixation in brain banking: a systematic review.Acta Neuropathol Commun. 2019 Sep 5;7(1):146. doi: 10.1186/s40478-019-0799-y. Acta Neuropathol Commun. 2019. PMID: 31488214 Free PMC article.
-
Lung transplantation, ex-vivo reconditioning and regeneration: state of the art and perspectives.J Thorac Dis. 2018 Jul;10(Suppl 20):S2423-S2430. doi: 10.21037/jtd.2018.04.151. J Thorac Dis. 2018. PMID: 30123580 Free PMC article. Review.
-
Thoracic organ machine perfusion: A review of concepts with a focus on reconditioning therapies.Front Transplant. 2023 Mar 22;2:1060992. doi: 10.3389/frtra.2023.1060992. eCollection 2023. Front Transplant. 2023. PMID: 38993918 Free PMC article. Review.
References
-
- Egan T.M., Lambert C.J., Jr., Reddick R. A strategy to increase the donor pool: use of cadaver lungs for transplantation. Ann. Thorac. Surg. 1991;52:1113–1120. discussion 1120–1111. - PubMed
-
- Hornby K., Ross H., Keshavjee S. Non-utilization of hearts and lungs after consent for donation: a Canadian multicentre study. Can. J. Anaesth. 2006;53:831–837. - PubMed
-
- Lindstedt S., Dellgren G., Iversen M. Pulmonary retransplantation in the nordic countries. Ann. Thorac. Surg. 2015;99:1781–1787. - PubMed
-
- de Antonio D.G., Marcos R., Laporta R. Results of clinical lung transplant from uncontrolled non-heart-beating donors. J. Heart Lung Transpl. 2007;26:529–534. - PubMed
-
- Steen S., Sjoberg T., Pierre L. Transplantation of lungs from a non-heart-beating donor. Lancet. 2001;357:825–829. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
