

Dynamic chronic rectal obstruction causing a severe colonic dilatation in a cat
- PMID: 28839947
- PMCID: PMC5565026
- DOI: 10.1177/2055116917725222
Dynamic chronic rectal obstruction causing a severe colonic dilatation in a cat
Abstract
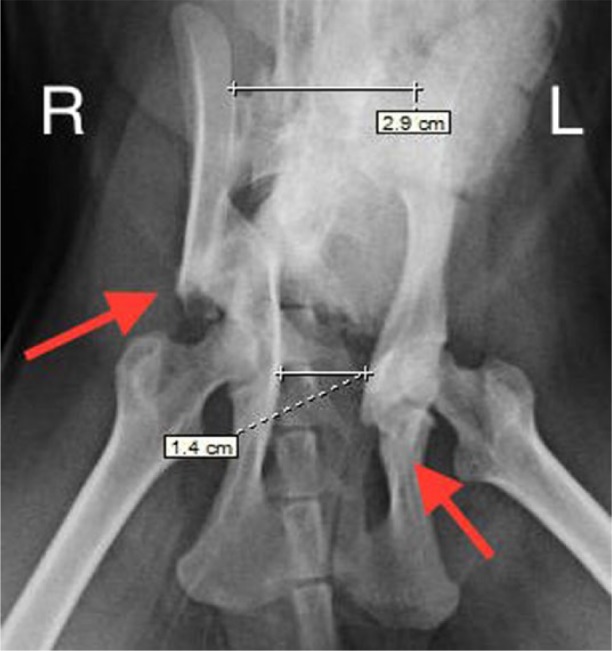
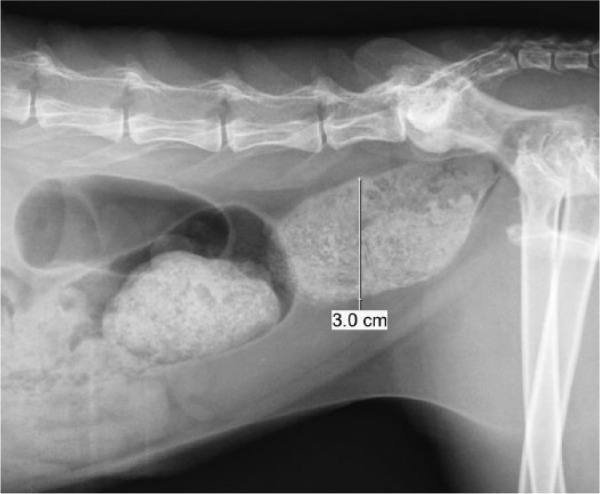
Case summary: A 5-year-old male neutered domestic shorthair cat was presented to our referral centre with a 13 month history of chronic tenesmus due to malunion of the right caudal iliac body. Constipation and pelvic canal stenosis were initially addressed by the referring veterinarian with a right femoral head and neck excision and a right acetabulectomy without observable clinical improvement. At admission, abdominal radiographs revealed severe colonic distension and a narrowed pelvic canal caused by the right proximal femur. Rectal examination and colonography revealed a dynamic compression of the rectum, which worsened with femoral abduction and improved with femoral adduction. A right hindlimb amputation was performed to relieve the obstruction. The cat defaecated 2 days postoperatively and was discharged uneventfully. Neither faecal tenesmus nor dyschaezia were observed over the following 10 months.
Relevance and novel information: The dynamic nature of the rectal obstruction most likely prevented the development of an irreversible colonic dilatation leading to a megacolon. This is the first report describing a chronic dynamic rectal compression, which was successfully managed with a right hindlimb amputation without the need for subtotal colectomy.
Conflict of interest statement
Conflict of interest: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures





References
-
- Yam P. Decision making in the management of constipation in the cat. In Pract 1997; 19: 434–440.
-
- Foley P. Constipation, tenesmus, dyschezia, and fecal incontinence. In: Ettinger SJ, Feldman EC, Côte E. (eds). Textbook of veterinary internal medicine. 8th ed. Philadelphia, PA: WB Saunders, 2017, pp 171–174.
-
- Bertoy RW. Megacolon in the cat. Vet Clin North Am Small Anim Pract 2002; 32: 901–915. - PubMed
-
- Washabau RJ, Hasler AG. Constipation, obstipation and megacolon. In: August JR. (ed). Consultations in feline internal medicine. 3rd ed. Philadelphia, PA: Saunders, 1997, pp 104–111.
-
- Hamilton MH, Evans DA, Langley-Hobbs SJ. Feline ilial fractures: assessment of screw loosening and pelvic canal narrowing after lateral plating. Vet Surg 2009; 38: 326–333. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous