

Assessment of Mediastinal Tumors Using SUVmax and Volumetric Parameters on FDG-PET/CT
- PMID: 28840135
- PMCID: PMC5221681
- DOI: 10.22038/aojnmb.2016.7996
Assessment of Mediastinal Tumors Using SUVmax and Volumetric Parameters on FDG-PET/CT
Abstract
Objectives: This study aimed to evaluate the role of pretreatment SUVmax and volumetric FDG positron emission tomography (PET) parameters in the differentiation between benign and malignant mediastinal tumors. In addition, we investigated whether pretreatment SUVmax and volumetric FDG-PET parameters could distinguish thymomas from thymic carcinomas, and low-risk from high-risk thymomas.
Methods: This study was conducted on 52 patients with mediastinal tumors undergoing FDG-PET/CT. Histological examination indicated that 29 mediastinal tumors were benign, and 23 cases were malignant. To obtain quantitative PET/CT parameters, we determined the maximum standardized uptake value (SUVmax), volumetric parameters, metabolic tumor volume (MTV), and total lesion glycolysis (TLG) for primary tumors using SUVmax cut-off value of 2.5. SUVmax, MTV and TLG of benign and malignant tumors were compared using the Mann-Whitney U test. Moreover, receiver-operating curve (ROC) analysis was applied to identify the cut-off values of SUVmax, MTV and TLG for the accurate differentiation of benign and malignant tumors. SUVmax, MTV and TLG were compared between thymomas and thymic carcinomas, as well as low-risk and high-risk thymomas.
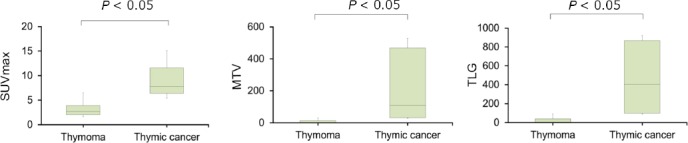
Results: Mean SUVmax, MTV and TLG of malignant mediastinal tumors were significantly higher compared to benign tumors (P<0.001). Sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of SUVmax were 78.2%, 86.2%, 82.6%, 81.8%, and 83.3%, respectively. These values were estimated at 82.6%, 96.6%, 90.4%, 95%, and 87.5% for MTV and TLG, respectively. Additionally, optimal cut-off values for the differentiation of benign and malignant mediastinal tumors were determined at 4.2 and 22.3 mL and 79.7 g for SUVmax, MTV and TLG, respectively. Mean SUVmax, MTV and TLG of thymic carcinomas were significantly higher compared to thymomas (P<0.01), while no significant differences were observed in the mean quantitative parameters between low-risk and high-risk thymomas.
Conclusion: Although SUVmax, MTV and TLG could not distinguish between low-risk and high-risk thymomas, these parameters might be able to differentiate benign tumors from malignant mediastinal tumors noninvasively. These parameters could be used to distinguish between thymomas and thymic carcinomas as well. Therefore, FDG-PET/CT parameters seem to be accurate indices for the detection of malignant mediastinal tumors.
Keywords: FDG-PET/CT; Mediastinal tumor; Metabolic tumor volume; Total lesion glycolysis.
Figures





References
-
- Strollo DC, Rosado de Christenson ML, Jett JR. Primary mediastinal tumors. Part 1:Tumors of the anterior mediastinum. Chest. 1997;112(2):511–22. - PubMed
-
- Okumura M, Ohta M, Tateyama H, Nakagawa K, Matsumura A, Maeda H, et al. The World Health Organization histologic classification system reflects the oncologic behavior of thymoma:a clinical study of 273 patients. Cancer. 2002;94(3):624–32. - PubMed
-
- Okumura M, Miyoshi S, Fujii Y, Takeuchi Y, Shiono H, Inoue M, et al. Clinical and functional significance of WHO classification on human thymic epithelial neoplasms:a study of 146 consecutive tumors. Am J Surg Pathol. 2001;25(1):103–10. - PubMed
-
- Chen G, Marx A, Chen WH, Yong J, Puppe B, Stroebel P, et al. New WHO histologic classification predicts prognosis of thymic epithelial tumors:a clinicopathologic study of 200 thymoma cases from China. Cancer. 2002;95(2):420–9. - PubMed
-
- Marchevsky AM, Gupta R, McKenna RJ, Wick M, Moran C, Zakowski MF, et al. Evidence-based pathology and the pathologic evaluation of thymomas:the world health organization classification can be simplified into only 3 categories other than thymic carcinoma. Cancer. 2008;112(12):2780–8. - PubMed
LinkOut - more resources
Full Text Sources