Size-based quality-informed framework for quantitative optimization of pediatric CT
- PMID: 28840168
- PMCID: PMC5565677
- DOI: 10.1117/1.JMI.4.3.031209
Size-based quality-informed framework for quantitative optimization of pediatric CT
Abstract
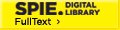
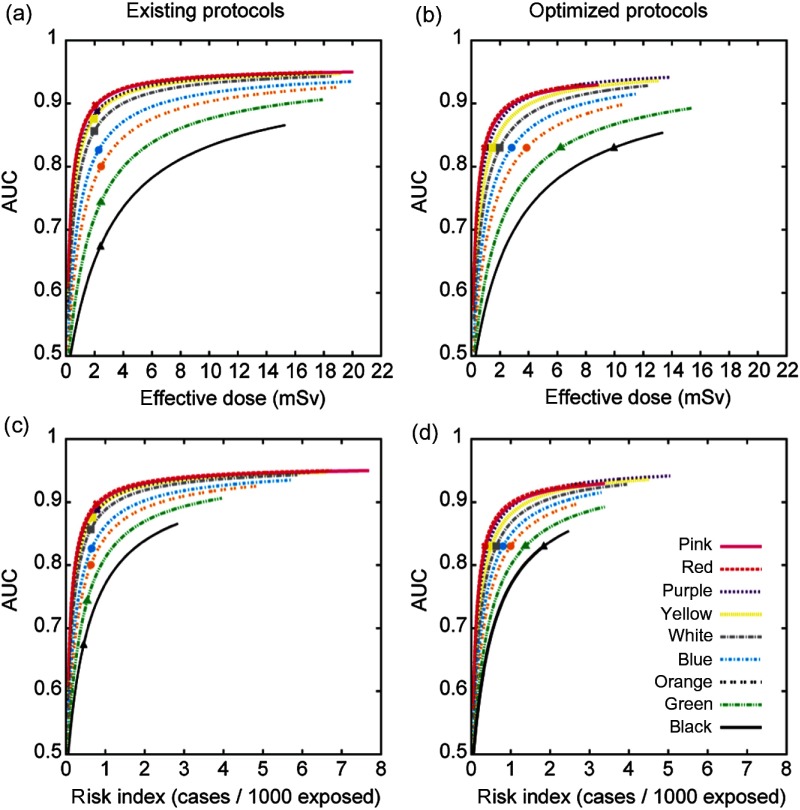
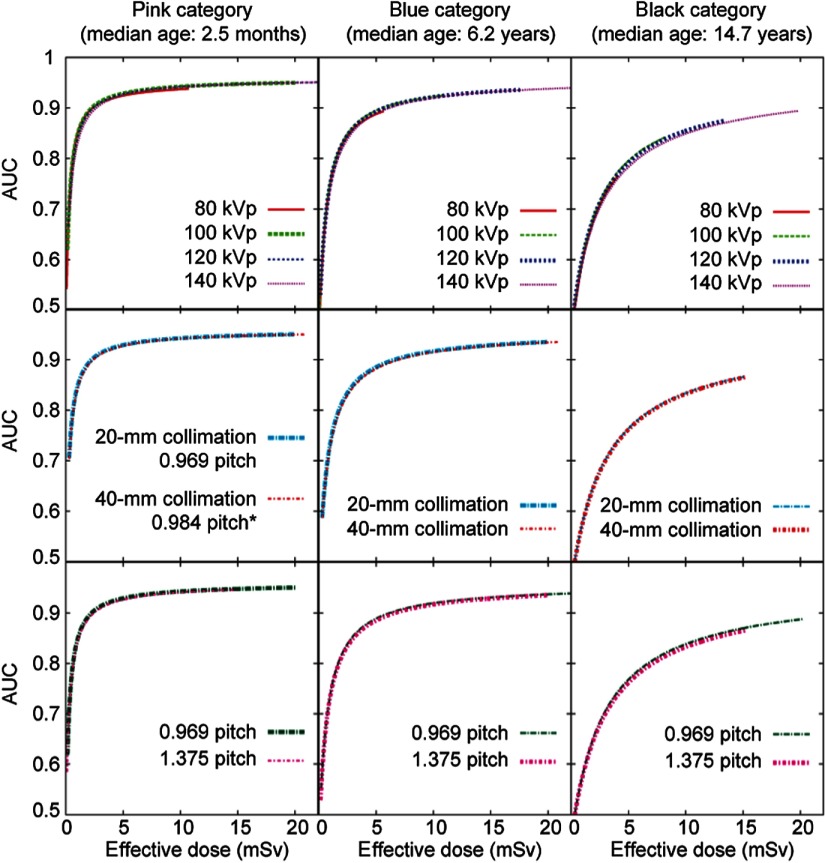
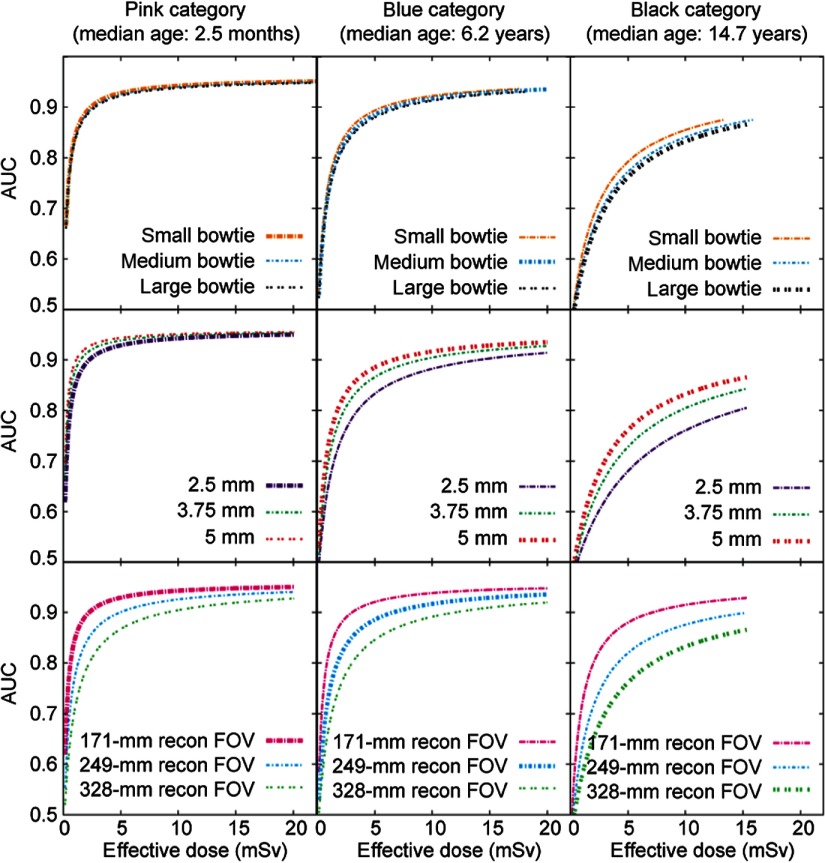
The purpose of this study was to formulate a systematic, evidence-based method to relate quantitative diagnostic performance to radiation dose, enabling a multidimensional system to optimize computed tomography imaging across pediatric populations. Based on two prior foundational studies, radiation dose was assessed in terms of organ doses, effective dose ([Formula: see text]), and risk index for 30 patients within nine color-coded pediatric age-size groups as a function of imaging parameters. The cases, supplemented with added noise and simulated lesions, were assessed in terms of nodule detection accuracy in an observer receiving operating characteristic study. The resulting continuous accuracy-dose relationships were used to optimize individual scan parameters. Before optimization, the nine protocols had a similar [Formula: see text] of [Formula: see text] with accuracy decreasing from 0.89 for the youngest patients to 0.67 for the oldest. After optimization, a consistent target accuracy of 0.83 was established for all patient categories with [Formula: see text] ranging from 1 to 10 mSv. Alternatively, isogradient operating points targeted a consistent ratio of accuracy-per-unit-dose across the patient categories. The developed model can be used to optimize individual scan parameters and provide for consistent diagnostic performance across the broad range of body sizes in children.
Keywords: children; computed tomography; diagnostic accuracy; image quality; lung nodule; pediatric; radiation dose; size-specific protocols.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources