

Plain radiography in patients treated with intrathecal drug delivery using an implantable pump device
- PMID: 28840489
- PMCID: PMC5621993
- DOI: 10.1007/s13244-017-0568-z
Plain radiography in patients treated with intrathecal drug delivery using an implantable pump device
Abstract
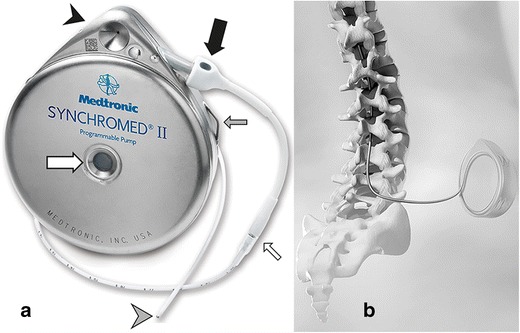
Objectives: Intrathecal drug administration using an implanted pump system is well established in intractable spasticity and pain. However, despite continuous advancements in manufacturing technology, adverse events related to the pump and catheter still occur. Most of them, such as migration, damage, disconnection and occlusion, are related to the spinal catheter. The aim of this overview is to update radiologists on how plain radiography of the implanted delivery system for intrathecal drug administration should be interpreted and to increase awareness for the need of urgent and timely multidisciplinary troubleshooting.
Methods: Plain radiographic images of patients treated with intrathecal drug administration using an implantable drug delivery system were analysed in a multidisciplinary setting at our (university) referral centre for complications in intrathecal drug administration.
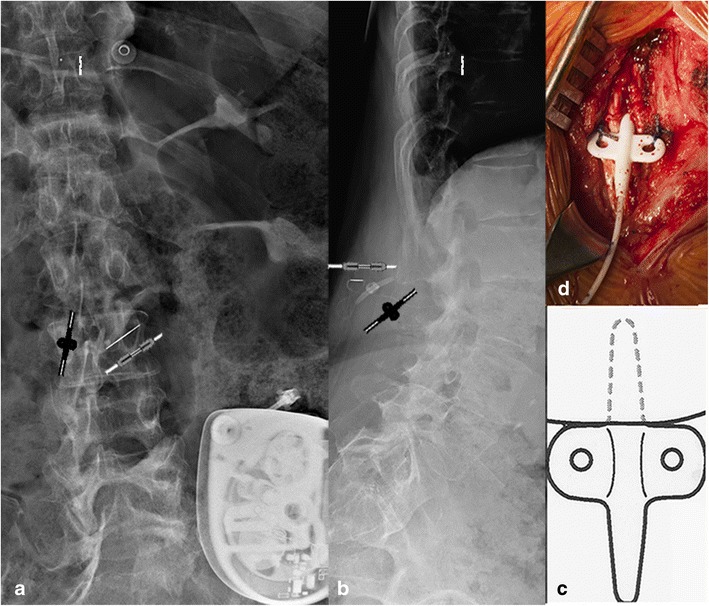
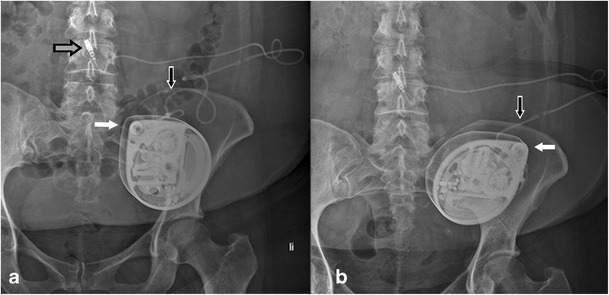
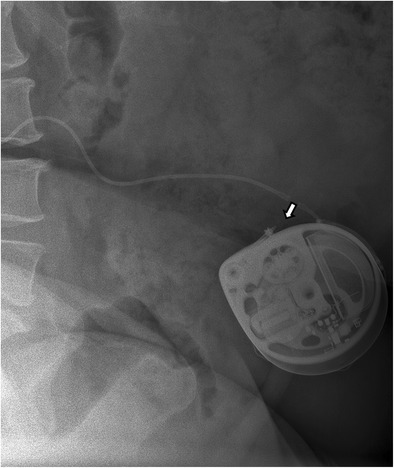
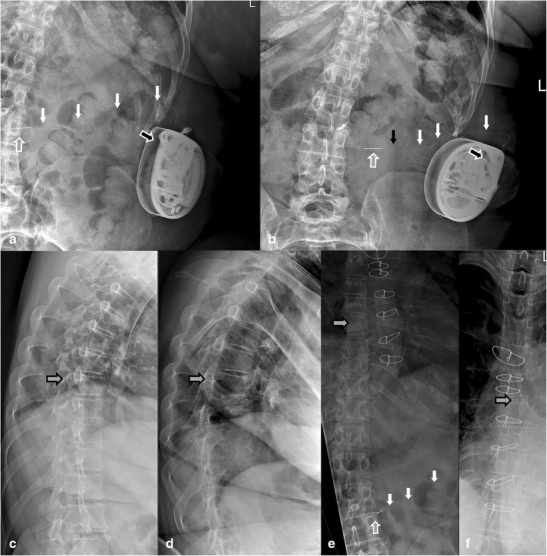
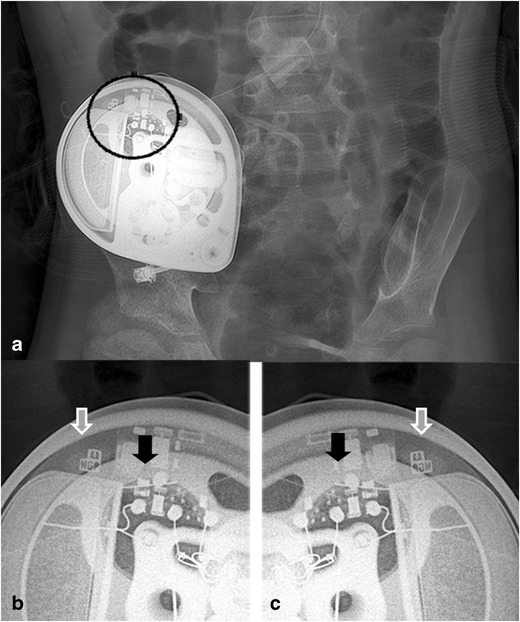
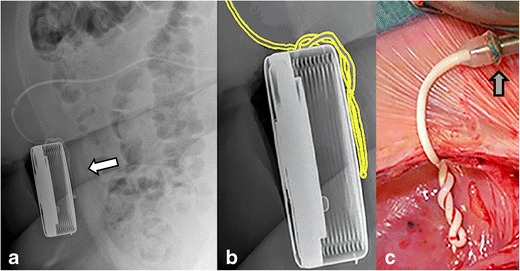
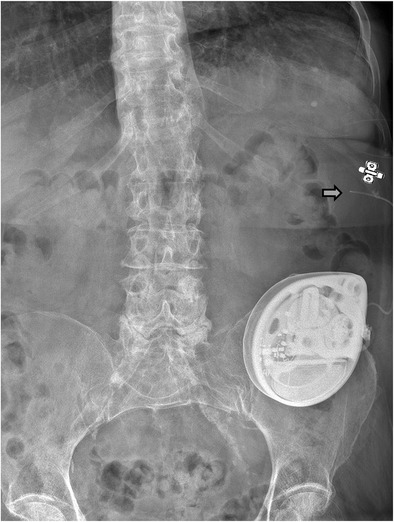
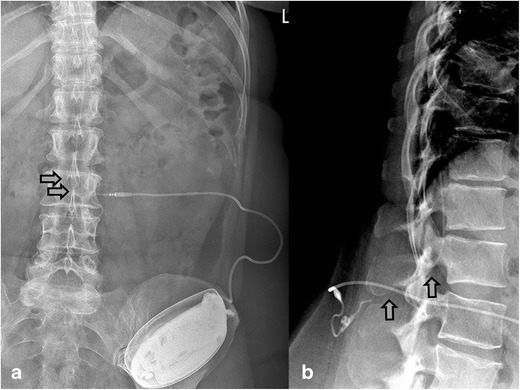
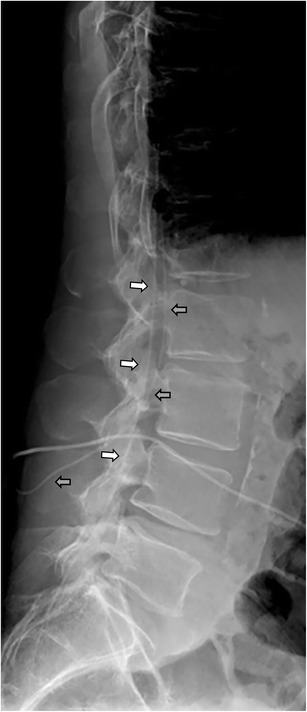
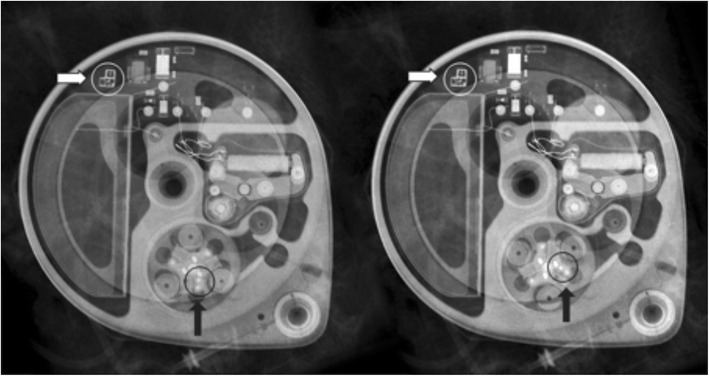
Results: Examples of catheter-related adverse events are described and a proposal is made for stepwise interpretation of standard plain radiographic images.
Conclusions: Plain radiological images are the mainstay for the diagnosis of catheter-related adverse events in intrathecal drug delivery. Radiologists play an important role in an early diagnosis. An awareness of abnormal radiological findings seems important to avoid a life-threatening withdrawal syndrome.
Teaching points: • Untimely cessation of intrathecal drug delivery can lead to a life-threatening withdrawal syndrome. • Initially mild symptoms can lead to an exacerbation of a withdrawal syndrome. • Most intrathecal catheter-related problems are visible on plain radiography. • Common causes of catheter problems are migration, lacerations, occlusion and disconnection. • Knowledge on implanted intrathecal catheters is crucial for interpretation of plain radiography.
Keywords: Adverse events; Diagnostic imaging; Implantable infusion pumps; Radiography; Spinal infusions.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
