

Classification and Current Management of Inner Ear Malformations
- PMID: 28840850
- PMCID: PMC5635626
- DOI: 10.4274/balkanmedj.2017.0367
Classification and Current Management of Inner Ear Malformations
Abstract
Morphologically congenital sensorineural hearing loss can be investigated under two categories. The majority of congenital hearing loss causes (80%) are membranous malformations. Here, the pathology involves inner ear hair cells. There is no gross bony abnormality and, therefore, in these cases high-resolution computerized tomography and magnetic resonance imaging of the temporal bone reveal normal findings. The remaining 20% have various malformations involving the bony labyrinth and, therefore, can be radiologically demonstrated by computerized tomography and magnetic resonance imaging. The latter group involves surgical challenges as well as problems in decision-making. Some cases may be managed by a hearing aid, others need cochlear implantation, and some cases are candidates for an auditory brainstem implantation (ABI). During cochlear implantation, there may be facial nerve abnormalities, cerebrospinal fluid leakage, electrode misplacement or difficulty in finding the cochlea itself. During surgery for inner ear malformations, the surgeon must be ready to modify the surgical approach or choose special electrodes for surgery. In the present review article, inner ear malformations are classified according to the differences observed in the cochlea. Hearing and language outcomes after various implantation methods are closely related to the status of the cochlear nerve, and a practical classification of the cochlear nerve deficiency is also provided.
Keywords: Inner ear malformations; classification; cochlear hypoplasia; cochleovestibular malformations; incomplete partition; radiology surgery.; treatment.
Conflict of interest statement
Figures







References
-
- Sennaroglu L. Cochlear implantation in inner ear malformations-a review article. Cochlear Implants Int. 2010;11:4–41. - PubMed
-
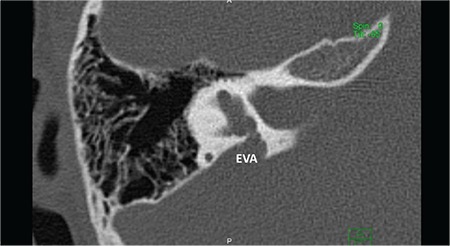
- Lemmerling MM, Mancuso AA, Antonelli PJ, Kubilis PS. Normal modiolus: CT appearance in patients with a large vestibular aqueduct. Radiology. 1997;204:213–9. - PubMed
-
- Sennaroglu L, Sennaroglu G, Ozgen B. Management of Inner ear Malformations, in Sataloff's Comprehensive Textbook of Otolaryngology. In: Sataloff RT, editor. JP Medical Publishers. 2015:91–106.
-
- Sennaroglu L. Histopathology of inner ear malformations: Do we have enough evidence to explain pathophysiology? Cochlear Implants Int. 2016;17:3–20. - PubMed
-
- Sennaroglu L, Colletti V, Manrique M, Laszig R, Offeciers E, Saeed S, et al. Auditory brainstem implantation in children and non-neurofibromatosis type 2 patients: a consensus statement. Otol Neurotol. 2011;32:187–91. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources