

Effect of time to initiation of postoperative radiation therapy on survival in surgically managed head and neck cancer
- PMID: 28841234
- PMCID: PMC5759768
- DOI: 10.1002/cncr.30939
Effect of time to initiation of postoperative radiation therapy on survival in surgically managed head and neck cancer
Abstract
Background: The objective of this study was to determine the effects of National Comprehensive Cancer Network (NCCN) guideline-adherent initiation of postoperative radiation therapy (PORT) and different time-to-PORT intervals on the overall survival (OS) of patients with head and neck squamous cell carcinoma (HNSCC).
Methods: The National Cancer Data Base was reviewed for the period of 2006-2014, and patients with HNSCC undergoing surgery and PORT were identified. Kaplan-Meier survival estimates, Cox regression analysis, and propensity score matching were used to determine the effects of initiating PORT within 6 weeks of surgery and different time-to-PORT intervals on survival.
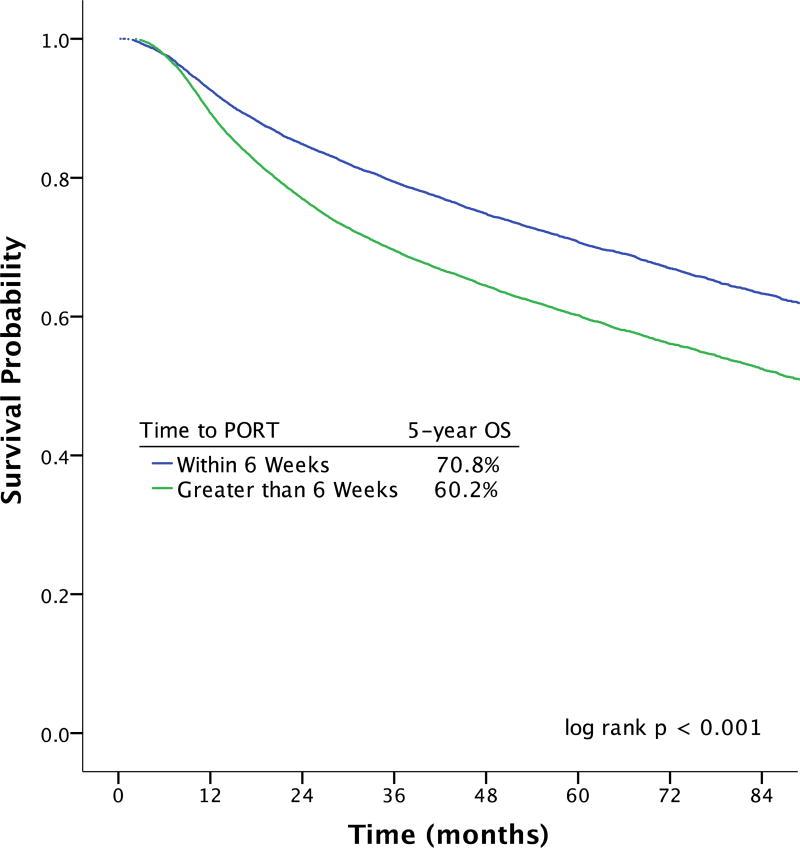
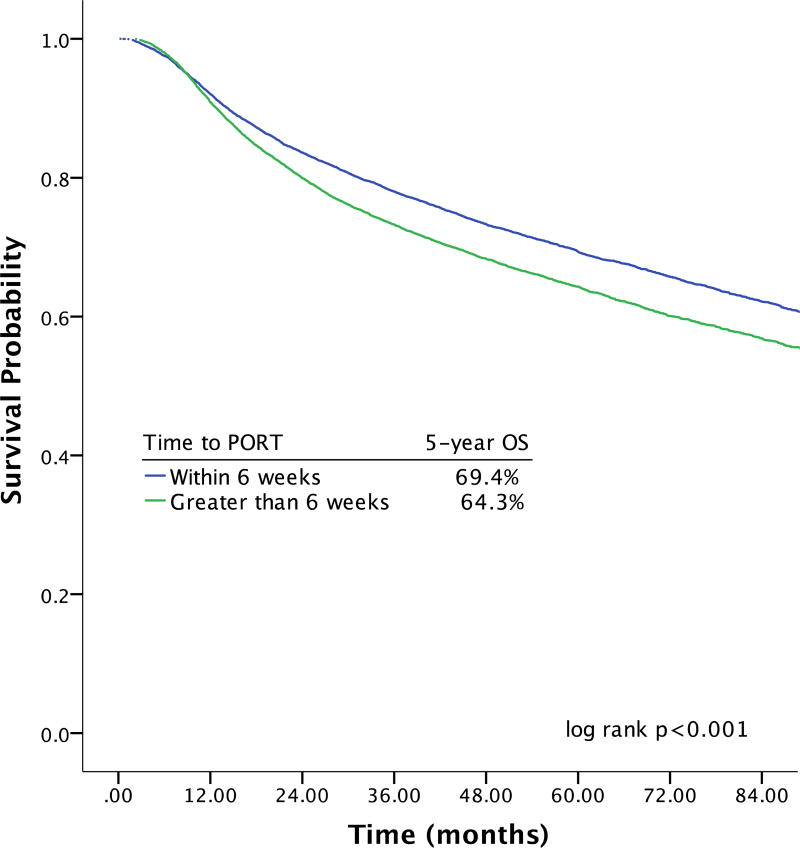
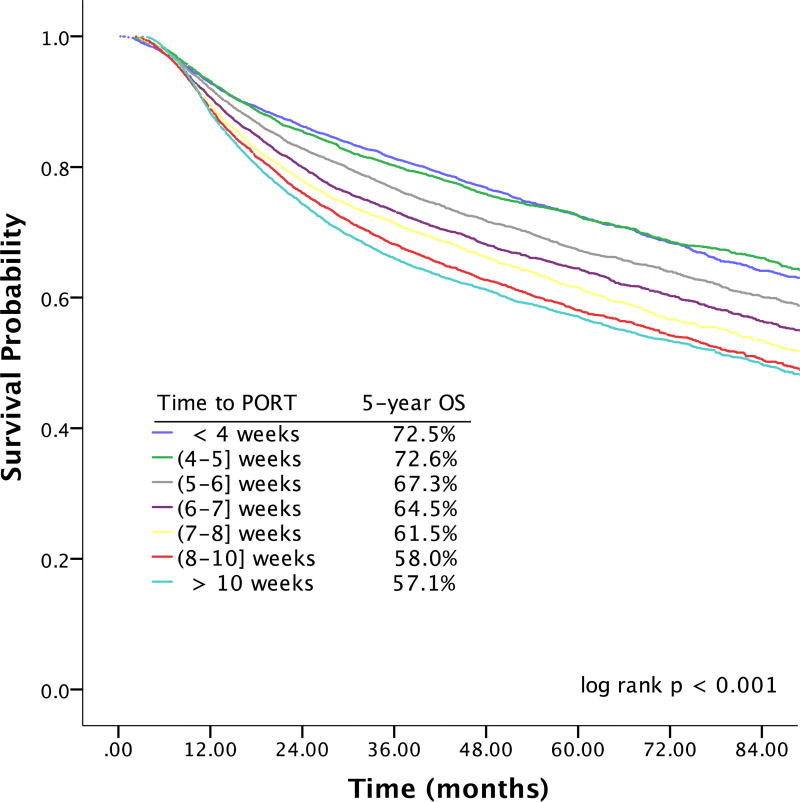
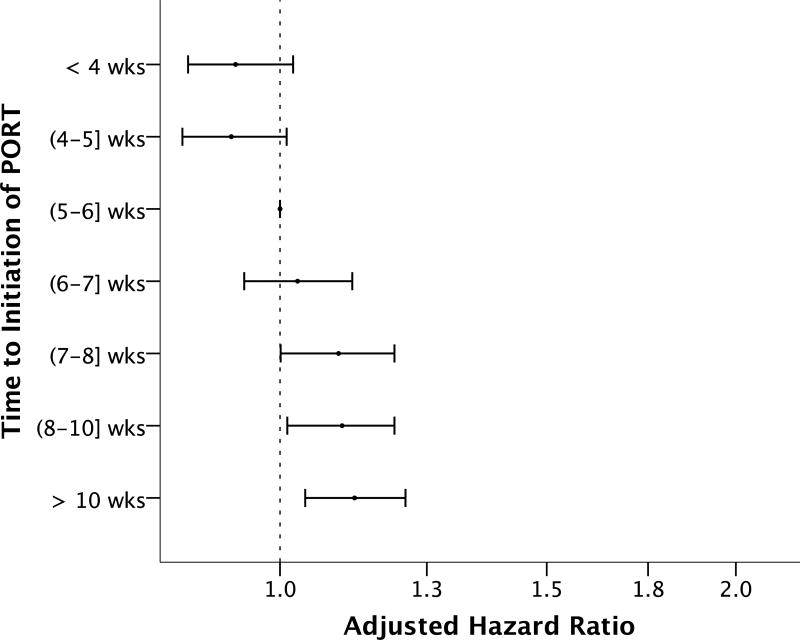
Results: This study included 41,291 patients. After adjustments for covariates, starting PORT >6 weeks postoperatively was associated with decreased OS (adjusted hazard ratio [aHR], 1.13; 99% confidence interval [CI], 1.08-1.19). This finding remained in the propensity score-matched subset (hazard ratio, 1.21; 99% CI, 1.15-1.28). In comparison with starting PORT 5 to 6 weeks postoperatively, initiating PORT earlier was not associated with improved survival (aHR for ≤ 4 weeks, 0.93; 99% CI, 0.85-1.02; aHR for 4-5 weeks, 0.92; 99% CI, 0.84-1.01). Increasing durations of delay beyond 7 weeks were associated with small, progressive survival decrements (aHR, 1.09, 1.10, and 1.12 for 7-8, 8-10, and >10 weeks, respectively).
Conclusions: Nonadherence to NCCN guidelines for initiating PORT within 6 weeks of surgery was associated with decreased survival. There was no survival benefit to initiating PORT earlier within the recommended 6-week timeframe. Increasing durations of delay beyond 7 weeks were associated with small, progressive survival decrements. Cancer 2017;123:4841-50. © 2017 American Cancer Society.
Keywords: National Cancer Data Base; National Comprehensive Cancer Network (NCCN) guidelines; head and neck cancer; postoperative radiation therapy; quality of care.
© 2017 American Cancer Society.
Conflict of interest statement
Disclosures/Conflicts of Interest: None
Figures
References
-
- Committee on Quality of Health Care in America IoM. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
-
- (NQMC). NQMC. [Accessed January 3 2017];Measure summary: Access: time to third next available appointment for an office visit. Available at: https://www.qualitymeasures.ahrq.gov/
-
- Kaplan G, Lopez MH, McGinnis JM. Transforming Healthcare Scheduling and Access: Getting to Now. Washington, DC: The National Academies Press; 2015. - PubMed
-
- Hewitt M, Simone J. National Cancer Policy Board: Ensuring Quality Cancer Care. Washington, DC: The National Academies Press; 1999. - PubMed
-
- Levit L, Balogh E, Nass S, Ganz P. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis. Washington, DC: The National Academies Press; 2013. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
