

Intelligence and Academic Achievement of Adolescents with Craniofacial Microsomia
- PMID: 28841618
- PMCID: PMC5657387
- DOI: 10.1097/PRS.0000000000003584
Intelligence and Academic Achievement of Adolescents with Craniofacial Microsomia
Abstract
Background: The authors compared the IQ and academic achievement of adolescents with craniofacial microsomia (cases) and unaffected children (controls). Among cases, the authors analyzed cognitive functioning by facial phenotype.
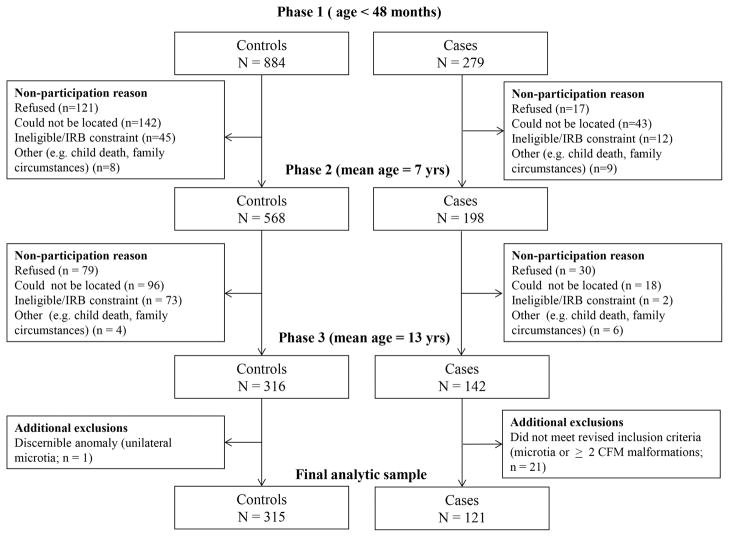
Methods: The authors administered standardized tests of intelligence, reading, spelling, writing, and mathematics to 142 cases and 316 controls recruited from 26 cities across the United States and Canada. Phenotypic classification was based on integrated data from photographic images, health history, and medical chart reviews. Hearing screens were conducted for all participants.
Results: After adjustment for demographics, cases' average scores were lower than those of controls on all measures, but the magnitude of differences was small (standardized effect sizes, -0.01 to -0.3). There was little evidence that hearing status modified case-control group differences (Wald p > 0.05 for all measures). Twenty-five percent of controls and 38 percent of cases were classified as having learning problems (adjusted OR, 1.5; 95 percent CI, 0.9 to 2.4). Comparison of cases with and without learning problems indicated that those with learning problems were more likely to be male, Hispanic, and to come from lower income, bilingual families. Analyses by facial phenotype showed that case-control group differences were largest for cases with both microtia and mandibular hypoplasia (effect sizes, -0.02 to -0.6).
Conclusions: The highest risk of cognitive-academic problems was observed in patients with combined microtia and mandibular hypoplasia. Developmental surveillance of this subgroup is recommended, especially in the context of high socioeconomic risk and bilingual families. Given the early stage of research on craniofacial microsomia and neurodevelopment, replication of these findings is needed.
Clinical question/level of evidence: Risk, II.
Figures
Comment in
-
Academic Capacities of Children With Cleft Lip and Palate.Ann Plast Surg. 2018 Dec;81(6):627-629. doi: 10.1097/SAP.0000000000001634. Ann Plast Surg. 2018. PMID: 30383586 No abstract available.
Similar articles
-
Hearing Loss in Children With Craniofacial Microsomia.Cleft Palate Craniofac J. 2017 Nov;54(6):656-663. doi: 10.1597/15-348. Epub 2016 Jul 26. Cleft Palate Craniofac J. 2017. PMID: 27458649
-
Neurodevelopment of Infants with and without Craniofacial Microsomia.J Pediatr. 2018 Jul;198:226-233.e3. doi: 10.1016/j.jpeds.2018.02.076. Epub 2018 Apr 22. J Pediatr. 2018. PMID: 29685618 Free PMC article.
-
Behavioral-Social Adjustment of Adolescents with Craniofacial Microsomia.Cleft Palate Craniofac J. 2018 May;55(5):664-675. doi: 10.1177/1055665617750488. Epub 2018 Jan 22. Cleft Palate Craniofac J. 2018. PMID: 29356621
-
Psychosocial and Health-Related Experiences of Individuals With Microtia and Craniofacial Microsomia and Their Families: Narrative Review Over 2 Decades.Cleft Palate Craniofac J. 2023 Sep;60(9):1090-1112. doi: 10.1177/10556656221091699. Epub 2022 Apr 5. Cleft Palate Craniofac J. 2023. PMID: 35382590 Free PMC article. Review.
-
Clinical care in craniofacial microsomia: a review of current management recommendations and opportunities to advance research.Am J Med Genet C Semin Med Genet. 2013 Nov;163C(4):271-82. doi: 10.1002/ajmg.c.31373. Epub 2013 Oct 16. Am J Med Genet C Semin Med Genet. 2013. PMID: 24132932 Review.
Cited by
-
[Obstructive sleep apnea in microtia children with maxillofacial dysostosis].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021 Apr;35(4):371-374;379. doi: 10.13201/j.issn.2096-7993.2021.04.020. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021. PMID: 33794641 Free PMC article. Review. Chinese.
-
Cognitive, Motor, and Language Development of Preschool Children With Craniofacial Microsomia.Cleft Palate Craniofac J. 2021 Sep;58(9):1169-1177. doi: 10.1177/1055665620980223. Epub 2020 Dec 16. Cleft Palate Craniofac J. 2021. PMID: 33322943 Free PMC article.
-
Methods and Challenges in a Cohort Study of Infants and Toddlers With Craniofacial Microsomia: The Clock Study.Cleft Palate Craniofac J. 2019 Aug;56(7):877-889. doi: 10.1177/1055665618821014. Epub 2019 Jan 8. Cleft Palate Craniofac J. 2019. PMID: 30621445 Free PMC article.
-
Speech, Language, and Communication Skills of Adolescents With Craniofacial Microsomia.Am J Speech Lang Pathol. 2019 Nov 19;28(4):1571-1581. doi: 10.1044/2019_AJSLP-19-0089. Epub 2019 Oct 3. Am J Speech Lang Pathol. 2019. PMID: 31580699 Free PMC article.
-
Academic achievement and needs of school-aged children born with selected congenital anomalies: A systematic review and meta-analysis.Birth Defects Res. 2021 Dec 1;113(20):1431-1462. doi: 10.1002/bdr2.1961. Epub 2021 Oct 21. Birth Defects Res. 2021. PMID: 34672115 Free PMC article.
References
-
- Poswillo D. The aetiology and pathogenesis of craniofcial deformity. Development. 1988;103:207–212. - PubMed
-
- Heike CL, Luquetti DV, Hing AV. Gene Reviews. Seattle, WA: University of Washington, Seattle; Mar 19, 2009. Craniofacial Microsomia Overview. http://www.ncbi.nlm.gov/books/NBK5199. 1993–2016. Updated Oct 9 2014. - PubMed
-
- Kjaer I. Human prenatal craniofacial development related to brain development under normal and pathologic conditions. Acta Odontol Scand. 1995;53(3):135–143. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
