

Delirium and Catatonia in Critically Ill Patients: The Delirium and Catatonia Prospective Cohort Investigation
- PMID: 28841632
- PMCID: PMC5678952
- DOI: 10.1097/CCM.0000000000002642
Delirium and Catatonia in Critically Ill Patients: The Delirium and Catatonia Prospective Cohort Investigation
Abstract
Objectives: Catatonia, a condition characterized by motor, behavioral, and emotional changes, can occur during critical illness and appear as clinically similar to delirium, yet its management differs from delirium. Traditional criteria for medical catatonia preclude its diagnosis in delirium. Our objective in this investigation was to understand the overlap and relationship between delirium and catatonia in ICU patients and determine diagnostic thresholds for catatonia.
Design: Convenience cohort, nested within two ongoing randomized trials.
Setting: Single academic medical center in Nashville, TN.
Patients: We enrolled 136 critically ill patients on mechanical ventilation and/or vasopressors, randomized to two usual care sedation regimens.
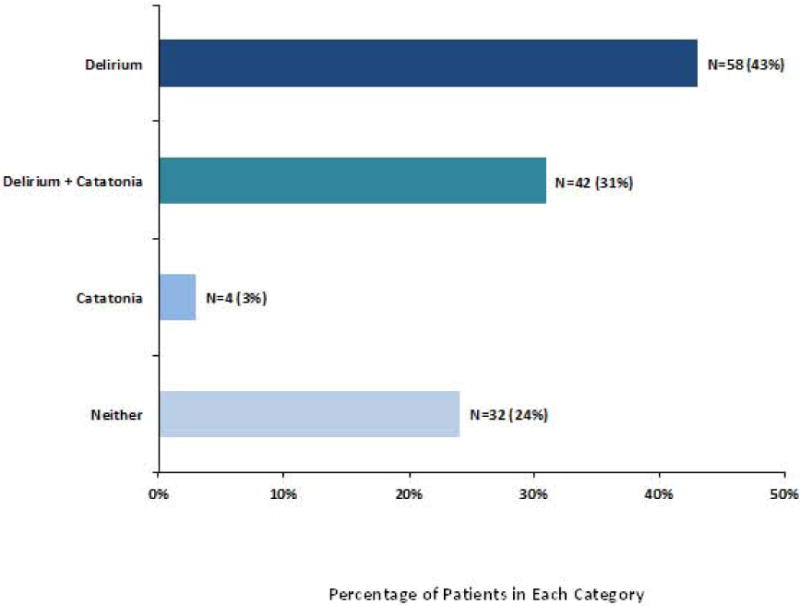
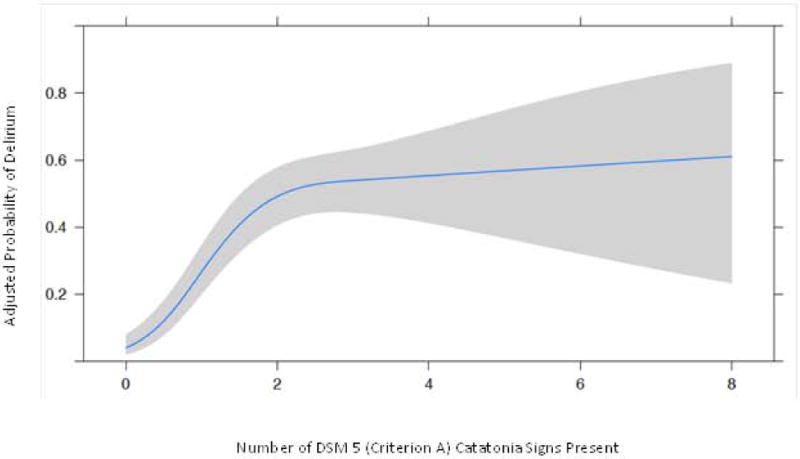
Measurements and main results: Patients were assessed for delirium and catatonia by independent and masked personnel using Confusion Assessment Method for the ICU and the Bush Francis Catatonia Rating Scale mapped to Diagnostic Statistical Manual 5 criterion A for catatonia. Of 136 patients, 58 patients (43%) had only delirium, four (3%) had only catatonia, 42 (31%) had both, and 32 (24%) had neither. In a logistic regression model, more catatonia signs were associated with greater odds of having delirium. For example, patient assessments with greater than or equal to three Diagnostic Statistical Manual 5 symptoms (75th percentile) had, on average, 27.8 times the odds (interquartile range, 12.7-60.6) of having delirium compared with patient assessments with zero Diagnostic Statistical Manual 5 criteria (25th percentile) present (p < 0.001). A cut-off of greater than or equal to 4 Bush Francis Catatonia Screening Instrument items was both sensitive (91%; 95% CI, 82.9-95.3) and specific (91%; 95% CI, 87.6-92.9) for Diagnostic Statistical Manual 5 catatonia.
Conclusions: Given that about one in three patients had both catatonia and delirium, these data prompt reconsideration of Diagnostic Statistical Manual 5 criteria for "Catatonic Disorder Due to Another Medical Condition" that preclude diagnosing catatonia in the presence of delirium.
Conflict of interest statement
Conflicts of Interest: The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Catatonia, Delirium, and Critical Illness: A Diagnostic Statistical Manual 5 Mystery Partially Disentangled.Crit Care Med. 2017 Nov;45(11):1953-1954. doi: 10.1097/CCM.0000000000002674. Crit Care Med. 2017. PMID: 29028701 No abstract available.
-
Deepening the Understanding of the Psychomotor Response to Critical Illness.Crit Care Med. 2018 Jul;46(7):e722. doi: 10.1097/CCM.0000000000003058. Crit Care Med. 2018. PMID: 29912121 No abstract available.
-
The authors reply.Crit Care Med. 2018 Jul;46(7):e722-e723. doi: 10.1097/CCM.0000000000003161. Crit Care Med. 2018. PMID: 29912122 Free PMC article. No abstract available.
Similar articles
-
Advanced Age Is Associated With Catatonia in Critical Illness: Results From the Delirium and Catatonia Prospective Cohort Investigation.Front Psychiatry. 2021 Nov 19;12:673166. doi: 10.3389/fpsyt.2021.673166. eCollection 2021. Front Psychiatry. 2021. PMID: 34867501 Free PMC article.
-
The Preschool Confusion Assessment Method for the ICU: Valid and Reliable Delirium Monitoring for Critically Ill Infants and Children.Crit Care Med. 2016 Mar;44(3):592-600. doi: 10.1097/CCM.0000000000001428. Crit Care Med. 2016. PMID: 26565631 Free PMC article.
-
Do patients of delirium have catatonic features? An exploratory study.Psychiatry Clin Neurosci. 2014 Aug;68(8):644-51. doi: 10.1111/pcn.12168. Epub 2014 Apr 13. Psychiatry Clin Neurosci. 2014. PMID: 24521083
-
Catatonia in the ICU: an important and underdiagnosed cause of altered mental status. a case series and review of the literature*.Crit Care Med. 2014 Mar;42(3):e234-41. doi: 10.1097/CCM.0000000000000053. Crit Care Med. 2014. PMID: 24275514 Review.
-
Distribution and frequency of clinical criteria and rating scales for diagnosis and assessment of catatonia in different study types.Schizophr Res. 2024 Jan;263:93-98. doi: 10.1016/j.schres.2022.12.019. Epub 2023 Jan 5. Schizophr Res. 2024. PMID: 36610862
Cited by
-
Persistent catatonia following epileptic seizures: a case report and systematic literature search.BMC Psychiatry. 2018 Oct 29;18(1):350. doi: 10.1186/s12888-018-1935-0. BMC Psychiatry. 2018. PMID: 30373550 Free PMC article.
-
Pseudodelirium: Psychiatric Conditions to Consider on the Differential for Delirium.J Neuropsychiatry Clin Neurosci. 2021 Fall;33(4):356-364. doi: 10.1176/appi.neuropsych.20120316. Epub 2021 Aug 16. J Neuropsychiatry Clin Neurosci. 2021. PMID: 34392693 Free PMC article.
-
In-hospital catatonia, delirium, and coma and mortality: Results from the delirium and catatonia prospective cohort investigation.Schizophr Res. 2024 Jan;263:223-228. doi: 10.1016/j.schres.2023.07.031. Epub 2023 Aug 12. Schizophr Res. 2024. PMID: 37580182 Free PMC article.
-
Electroconvulsive Therapy for Malignant Catatonia: A Case Report in the Intensive Care Unit.Cureus. 2025 May 8;17(5):e83714. doi: 10.7759/cureus.83714. eCollection 2025 May. Cureus. 2025. PMID: 40486423 Free PMC article.
-
A Case of Catatonia in a Man With COVID-19.Psychosomatics. 2020 Sep-Oct;61(5):556-560. doi: 10.1016/j.psym.2020.05.021. Epub 2020 May 27. Psychosomatics. 2020. PMID: 32605766 Free PMC article. No abstract available.
References
-
- Saddawi-Konefka D, Berg SM, Nejad SH, et al. Catatonia in the ICU: an important and underdiagnosed cause of altered mental status. a case series and review of the literature*. Crit Care Med. 2014;42(3):e234–241. - PubMed
-
- Grover S, Ghosh A, Ghormode D. Do patients of delirium have catatonic features? An exploratory study. Psychiatry Clin Neurosci. 2014;68(8):644–651. - PubMed
-
- Rizos DV, Peritogiannis V, Gkogkos C. Catatonia in the intensive care unit. Gen Hosp Psychiatry. 2011;33(1):e1–2. - PubMed
-
- Gelenberg AJ. The catatonic syndrome. Lancet. 1976;1(7973):1339–1341. - PubMed
-
- Milbrandt EB, Deppen S, Harrison PL, et al. Costs associated with delirium in mechanically ventilated patients. Crit Care Med. 2004;32(4):955–962. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
