

Maternal and perinatal outcome after previous caesarean section in rural Rwanda
- PMID: 28841838
- PMCID: PMC5574082
- DOI: 10.1186/s12884-017-1467-5
Maternal and perinatal outcome after previous caesarean section in rural Rwanda
Abstract
Background: Offering a trial of labor (ToL) after previous caesarean section (CS) is an important strategy to reduce short- and long-term morbidity associated with repeated CS. We compared maternal and perinatal outcomes between ToL and elective repeat caesarean section (ERCS) at a district hospital in rural Rwanda.
Methods: Audit of women's records with one prior CS who delivered at Ruhengeri district hospital in Rwanda between June 2013 and December 2014.
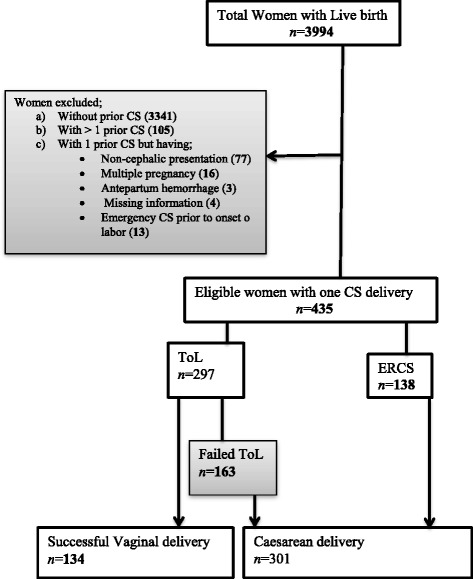
Results: Out of 4131 women who came for delivery, 435 (11%) had scarred uteri. ToL, which often started at home or at health centers without appropriate counseling, occurred in 297/435 women (68.3%), while 138 women (31.7%) delivered by ERCS. ToL was successful in 134/297 (45.1%) women. There were no maternal deaths. Twenty-eight out of all 435 women with a scarred uterus (6.4%) sustained severe acute maternal morbidity (puerperal sepsis, postpartum hemorrhage, uterine rupture), which was higher in women with ToL (n = 23, 7.7%) compared with women who had an ERCS (n = 5, 3.6%): adjusted odds ration (aOR) 1.4 (95% CI 1.2-5.4). There was no difference in neonatal admissions between women who underwent ToL (n = 64/297; 21.5%) and those who delivered by ERCS (n = 35/138; 25.4%: aOR 0.8; CI 0.5-1.6). The majority of admissions were due to perinatal asphyxia that occurred more often in infants whose mothers underwent ToL (n = 40, 13.4%) compared to those who delivered by ERCS (n = 15, 10.9%: aOR 1.9; CI 1.6-3.6). Perinatal mortality was similar among infants whose mothers had ToL (n = 8; 27/1000 ToLs) and infants whose mothers underwent ERCS (n = 4; 29/1000 ERCSs).
Conclusions: A considerable proportion of women delivering at a rural Rwandan hospital had scarred uteri. Severe acute maternal morbidity was higher in the ToL group, perinatal mortality did not differ. ToL took place under suboptimal conditions: access for women with scarred uteri into a facility with 24-h surgery should be guaranteed to increase the safety of ToL.
Keywords: Elective repeat caesarean delivery; Maternal morbidity; Sub-Saharan Africa; Trial of labor; Vaginal birth after caesarean section.
Conflict of interest statement
Ethics approval and consent to participate
Ethical clearance was obtained from the national ethical committee (N°582/RNEC/2013). All data entered into the database were anonymized and could not be traced back to individual participants. The medical director of Ruhengeri hospital gave permission.
Consent for publication
Consent to publish this manuscript from the participants was deemed not applicable since the manuscript does not contain any individual person data.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Maternal and perinatal outcomes associated with a trial of labour after previous caesarean section in sub-Saharan countries.BJOG. 2016 Dec;123(13):2147-2155. doi: 10.1111/1471-0528.13615. Epub 2015 Sep 16. BJOG. 2016. PMID: 26374554
-
Neonatal morbidity after elective repeat cesarean section and trial of labor.Pediatrics. 1997 Sep;100(3 Pt 1):348-53. doi: 10.1542/peds.100.3.348. Pediatrics. 1997. PMID: 9282704
-
Planned mode of delivery after previous cesarean section and short-term maternal and perinatal outcomes: A population-based record linkage cohort study in Scotland.PLoS Med. 2019 Sep 24;16(9):e1002913. doi: 10.1371/journal.pmed.1002913. eCollection 2019 Sep. PLoS Med. 2019. PMID: 31550245 Free PMC article.
-
[Maternal benefits and risks of trial of labor versus elective repeat caesarean delivery in women with a previous caesarean delivery].J Gynecol Obstet Biol Reprod (Paris). 2012 Dec;41(8):708-26. doi: 10.1016/j.jgyn.2012.09.028. Epub 2012 Nov 14. J Gynecol Obstet Biol Reprod (Paris). 2012. PMID: 23159201 Review. French.
-
SOGC clinical practice guidelines. Guidelines for vaginal birth after previous caesarean birth. Number 155 (Replaces guideline Number 147), February 2005.Int J Gynaecol Obstet. 2005 Jun;89(3):319-31. doi: 10.1016/j.ijgo.2005.03.015. Int J Gynaecol Obstet. 2005. PMID: 16001462 Review.
Cited by
-
Risk Factors Associated with Uterine Rupture and Dehiscence: A Cross-Sectional Canadian Study.Rev Bras Ginecol Obstet. 2021 Nov;43(11):820-825. doi: 10.1055/s-0041-1739461. Epub 2021 Dec 6. Rev Bras Ginecol Obstet. 2021. PMID: 34872139 Free PMC article.
-
Impact of Medical Doctors Global Health and Tropical Medicine on decision-making in caesarean section: a pre- and post-implementation study in a rural hospital in Malawi.Hum Resour Health. 2020 Nov 9;18(1):87. doi: 10.1186/s12960-020-00516-5. Hum Resour Health. 2020. PMID: 33168014 Free PMC article.
-
Predictors of successful trial of labor after cesarean section (TOLAC) in women with one prior transverse cesarean section at Tertiary Hospitals in northwest Ethiopia: a multicenter study.BMC Pregnancy Childbirth. 2024 Apr 5;24(1):240. doi: 10.1186/s12884-024-06432-z. BMC Pregnancy Childbirth. 2024. PMID: 38580911 Free PMC article.
-
Socioeconomic, demographic and obstetric determinants of maternal near miss in Africa: A systematic review.PLoS One. 2025 Feb 12;20(2):e0313897. doi: 10.1371/journal.pone.0313897. eCollection 2025. PLoS One. 2025. PMID: 39937712 Free PMC article.
-
Factors associated with successful vaginal birth after a cesarean section: a systematic review and meta-analysis.BMC Pregnancy Childbirth. 2019 Oct 17;19(1):360. doi: 10.1186/s12884-019-2517-y. BMC Pregnancy Childbirth. 2019. PMID: 31623587 Free PMC article.
References
-
- Vogel JP, Betrán AP, Vindevoghel N, Souza JP, Torloni MR, Zhang J. WHO multi-country survey on maternal and newborn Health Research network: use of the Robson classification to assess caesarean section trends in 21 countries: a secondary analysis of two WHO multicountry surveys. Lancet Glob Health. 2015;3(5):e260–e270. doi: 10.1016/S2214-109X(15)70094-X. - DOI - PubMed
-
- Briand V, Dumont A, Abrahamowicz M, Traore M, Watier L, Fournier P. Individual and institutional determinants of caesarean section in referral hospitals in Senegal and Mali: a cross-sectional epidemiological survey. BMC Pregnancy Childbirth. 2012;12:114. doi: 10.1186/1471-2393-12-114. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
