

Current clinical nutrition practices in critically ill patients in Latin America: a multinational observational study
- PMID: 28841885
- PMCID: PMC6389103
- DOI: 10.1186/s13054-017-1805-z
Current clinical nutrition practices in critically ill patients in Latin America: a multinational observational study
Abstract
Background: Malnutrition in critically ill adults in the intensive care unit (ICU) is associated with a significantly elevated risk of mortality. Adequate nutrition therapy is crucial to optimise outcomes. Currently, there is a paucity of such data in Latin America. Our aims were to characterise current clinical nutrition practices in the ICU setting in Latin America and evaluate whether current practices meet caloric and protein requirements in critically ill patients receiving nutrition therapy.
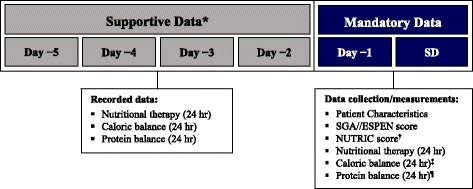
Methods: We conducted a cross-sectional, retrospective, observational study in eight Latin American countries (Argentina, Brazil, Chile, Colombia, Ecuador, Mexico, Panama, and Peru). Eligible patients were critically ill adults hospitalised in the ICU and receiving enteral nutrition (EN) and/or parenteral nutrition (PN) on the Screening Day and the previous day (day -1). Caloric and protein balance on day -1, nutritional status, and prescribed nutrition therapy were recorded. Multivariable logistic regression analysis was performed to identify independent predictors of reaching daily caloric and protein targets.
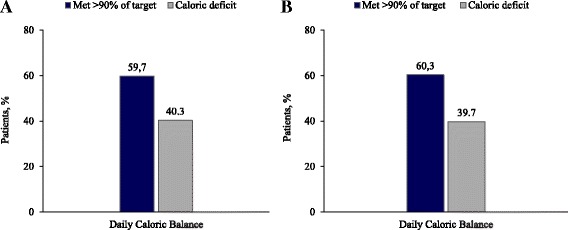
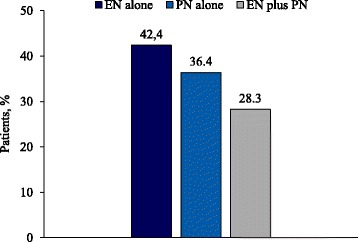
Results: The analysis included 1053 patients from 116 hospitals. Evaluation of nutritional status showed that 74.1% of patients had suspected/moderate or severe malnutrition according to the Subjective Global Assessment. Prescribed nutrition therapy included EN alone (79.9%), PN alone (9.4%), and EN + PN (10.7%). Caloric intake met >90% of the daily target in 59.7% of patients on day -1; a caloric deficit was present in 40.3%, with a mean (±SD) daily caloric deficit of -688.8 ± 455.2 kcal. Multivariable logistic regression analysis showed that combined administration of EN + PN was associated with a statistically significant increase in the probability of meeting >90% of daily caloric and protein targets compared with EN alone (odds ratio, 1.56; 95% confidence interval, 1.02-2.39; p = 0.038).
Conclusions: In the ICU setting in Latin America, malnutrition was highly prevalent and caloric intake failed to meet targeted energy delivery in 40% of critically ill adults receiving nutrition therapy. Supplemental administration of PN was associated with improved energy and protein delivery; however, PN use was low. Collectively, these findings suggest an opportunity for more effective utilisation of supplemental PN in critically ill adults who fail to receive adequate nutrition from EN alone.
Keywords: Caloric balance; Disease-related malnutrition; Enteral nutrition; Intensive care; Parenteral nutrition.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
The study protocol was approved by the local ethics committee or institutional review board at participating institutions in accordance with local regulations for non-interventional studies (Additional file 2). Where required by local regulations or ethics committee policy, written informed consent was obtained from each patient or family member before enrollment.
Consent for publication
Not applicable.
Competing interests
KPV, CMM, AAMA, VFT, GCCN, RERP, MIP, MITDC, and DLW have served on an advisory board for Fresenius Kabi. GCCN has served as a consultant for Global Mix Pharma. MITDC has served as an advisor for Abbot and Baxter and received honoraria for lectures from Abbott, Baxter, Fresenius Kabi, Nestlé, and Sanofi, and research support from Invictus. MIP has received honoraria for lectures from Fresenius Kabi. DLW has served as an advisor for Danone and received honoraria for lectures from Ache, B. Braun, Danone, and Fresenius Kabi.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- White JV, Guenter P, Jensen G, et al. Consensus Statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition) JPEN J Parenter Enteral Nutr. 2012;36:275–83. doi: 10.1177/0148607112440285. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
