

Immediate postpartum levonorgestrel intrauterine device insertion and breast-feeding outcomes: a noninferiority randomized controlled trial
- PMID: 28842126
- PMCID: PMC6040814
- DOI: 10.1016/j.ajog.2017.08.003
Immediate postpartum levonorgestrel intrauterine device insertion and breast-feeding outcomes: a noninferiority randomized controlled trial
Abstract
Background: Immediate postpartum levonorgestrel intrauterine device insertion is increasing in frequency in the United States, but few studies have investigated the effect of early placement on breast-feeding outcomes.
Objective: This study examined the effect of immediate vs delayed postpartum levonorgestrel intrauterine device insertion on breast-feeding outcomes.
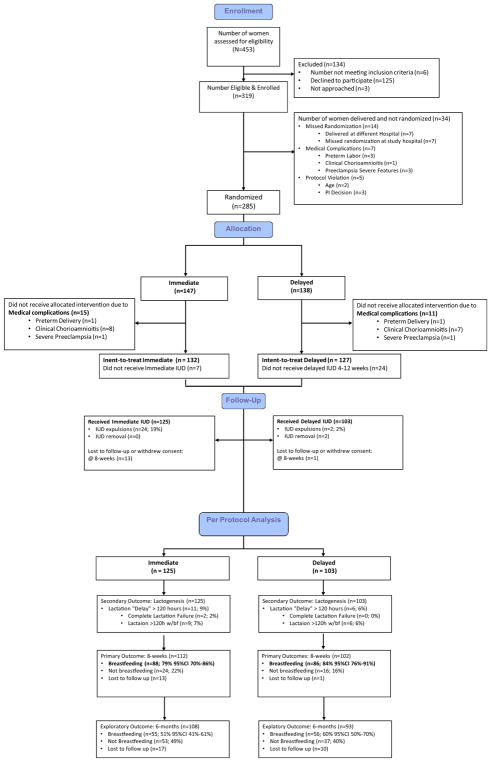
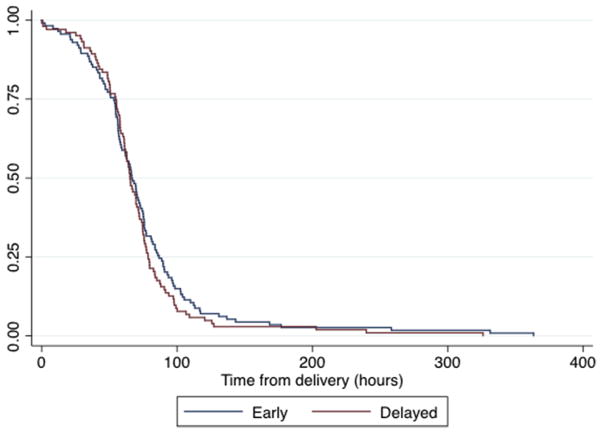
Study design: We conducted this noninferiority randomized controlled trial at the University of Utah and the University of New Mexico Health Sciences Centers from February 2014 through March 2016. Eligible women were pregnant and planned to breast-feed, spoke English or Spanish, were aged 18-40 years, and desired a levonorgestrel intrauterine device. Enrolled women were randomized 1:1 to immediate postpartum insertion or delayed insertion at 4-12 weeks' postpartum. Prespecified exclusion criteria included delivery <37.0 weeks' gestational age, chorioamnionitis, postpartum hemorrhage, contraindications to levonorgestrel intrauterine device insertion, and medical complications of pregnancy that could affect breast-feeding. We conducted per-protocol analysis as the primary approach, as it is considered the standard for noninferiority studies; we also report the alternative intent-to-treat analysis. We powered the study for the primary outcome, breast-feeding continuation at 8 weeks, to detect a 15% noninferiority margin between groups, requiring 132 participants in each arm. The secondary study outcome, time to lactogenesis, used a validated measure, and was analyzed by survival analysis and log rank test. We followed up participants for ongoing data collection for 6 months. Only the data analysis team was blinded to the intervention.
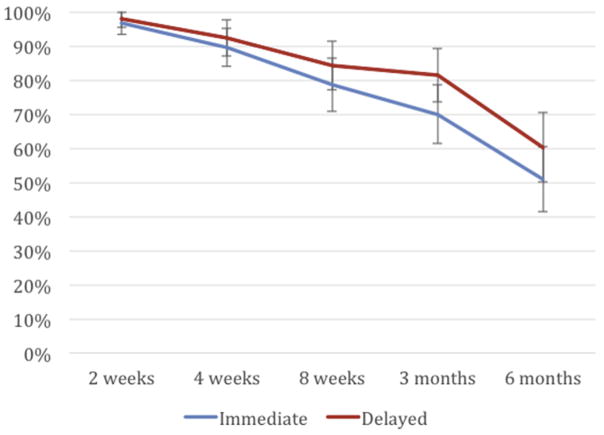
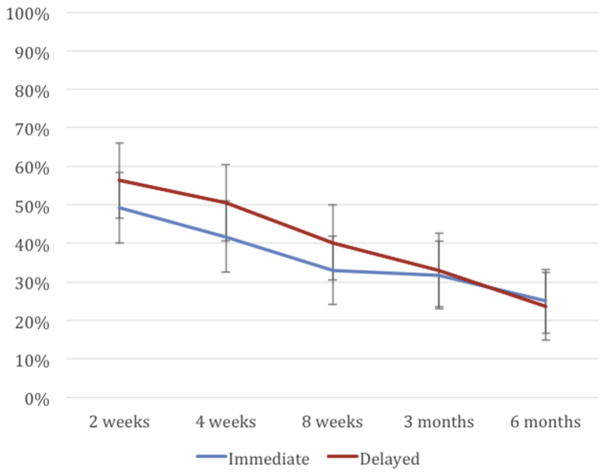
Results: We met the enrollment target with 319 participants, but lost 34 prior to randomization and excluded an additional 26 for medical complications prior to delivery. The final analytic sample included 132 in the immediate group and 127 in the delayed group. Report of any breast-feeding at 8 weeks in the immediate group (79%; 95% confidence interval, 70-86%) was noninferior to that of the delayed group (84%; 95% confidence interval, 76-91%). The 5% difference in breast-feeding continuation at 8 weeks between the groups fell within the noninferiority margin (95% confidence interval, -5.6 to 15%). Time to lactogenesis (mean ± SD) in the immediate group, 65.3 ± 25.7 hours, was noninferior to that of the delayed group, 63.6 ± 21.6 hours. The mean difference between groups was 1.7 hours (95% confidence interval, -4.8 to 8.2 hours), noninferior by log-rank test. A total of 24 intrauterine device expulsions occurred in the immediate group compared to 2 in the delayed group (19% vs 2%, P < .001), consistent with the known higher expulsion rate with immediate vs delayed postpartum intrauterine device insertion. No intrauterine device perforations occurred in either group.
Conclusion: Our results of noninferior breast-feeding outcomes between women with immediate and delayed postpartum levonorgestrel intrauterine device insertion suggest that immediate postpartum intrauterine device insertion is an acceptable option for women planning to breast-feed and use the levonorgestrel intrauterine device. Expulsion rates are higher with immediate postpartum levonorgestrel intrauterine device insertion compared to delayed insertion, but this disadvantage may be outweighed by the advantages of immediate initiation of contraception. Providers should offer immediate postpartum intrauterine device insertion to breast-feeding women planning to use the levonorgestrel intrauterine device.
Keywords: breast-feeding; contraception; immediate postpartum intrauterine device insertion; levonorgestrel intrauterine device.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Postplacental intrauterine device expulsion by 12 weeks: a prospective cohort study.Am J Obstet Gynecol. 2017 Dec;217(6):674.e1-674.e8. doi: 10.1016/j.ajog.2017.08.001. Epub 2017 Aug 19. Am J Obstet Gynecol. 2017. PMID: 28826801
-
Immediate postpartum intrauterine device and implant program outcomes: a prospective analysis.Am J Obstet Gynecol. 2017 Jul;217(1):51.e1-51.e7. doi: 10.1016/j.ajog.2017.03.015. Epub 2017 Mar 23. Am J Obstet Gynecol. 2017. PMID: 28342716
-
Lactogenesis and breastfeeding after immediate vs delayed birth-hospitalization insertion of etonogestrel contraceptive implant: a noninferiority trial.Am J Obstet Gynecol. 2023 Jan;228(1):55.e1-55.e9. doi: 10.1016/j.ajog.2022.08.012. Epub 2022 Aug 12. Am J Obstet Gynecol. 2023. PMID: 35964661 Clinical Trial.
-
Expulsion of intrauterine devices after postpartum placement by timing of placement, delivery type, and intrauterine device type: a systematic review and meta-analysis.Am J Obstet Gynecol. 2020 Aug;223(2):177-188. doi: 10.1016/j.ajog.2020.02.045. Epub 2020 Mar 3. Am J Obstet Gynecol. 2020. PMID: 32142826 Free PMC article.
-
The effect of early vs. delayed postpartum insertion of the LNG-IUS on breastfeeding continuation: a systematic review and meta-analysis of randomised controlled trials.Eur J Contracept Reprod Health Care. 2019 Oct;24(5):327-336. doi: 10.1080/13625187.2019.1665175. Epub 2019 Sep 13. Eur J Contracept Reprod Health Care. 2019. PMID: 31517549
Cited by
-
Risk factors for self-reported insufficient milk during the first 6 months of life: A systematic review.Matern Child Nutr. 2022 May;18 Suppl 3(Suppl 3):e13353. doi: 10.1111/mcn.13353. Epub 2022 Mar 28. Matern Child Nutr. 2022. PMID: 35343065 Free PMC article.
-
Intrauterine Device Expulsion After Postpartum Placement: A Systematic Review and Meta-analysis.Obstet Gynecol. 2018 Oct;132(4):895-905. doi: 10.1097/AOG.0000000000002822. Obstet Gynecol. 2018. PMID: 30204688 Free PMC article.
-
Postplacental Insertion of Levonorgestrel Intrauterine System Versus Copper Intrauterine Device: A Prospective Study.J Obstet Gynaecol India. 2021 Apr;71(2):150-155. doi: 10.1007/s13224-020-01409-2. Epub 2021 Jan 20. J Obstet Gynaecol India. 2021. PMID: 34149217 Free PMC article.
-
Utilisation, effectiveness, and safety of immediate postpartum intrauterine device insertion: a systematic literature review.BMJ Sex Reprod Health. 2023 Apr;49(2):e1. doi: 10.1136/bmjsrh-2022-201579. Epub 2022 Dec 9. BMJ Sex Reprod Health. 2023. PMID: 36600467 Free PMC article.
-
Breastfeeding and contraception counseling: a qualitative study.BMC Pregnancy Childbirth. 2022 Feb 25;22(1):154. doi: 10.1186/s12884-022-04451-2. BMC Pregnancy Childbirth. 2022. PMID: 35216562 Free PMC article.
References
-
- American Academy of Pediatrics Committee on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics. 2012;129:e827–41. - PubMed
-
- Dykes F, Moran VH. Infant and young child feeding: challenges to implementing a global strategy. Chichester (United Kingdom) and Ames (IA): Wiley-Blackwell; 2009.
-
- Centers for Disease Control and Prevention. [Accessed Oct. 10, 2016];Infant feeding practices study II and its year six follow up. Available at: http://www.cdc.gov/breastfeeding/data/ifps/results.htm.
-
- National Center for Health Statistics. Healthy People 2020 midcourse review. Hyattsville (MD): US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
