

Prospective Clinical Implementation of a Novel Magnetic Resonance Tracking Device for Real-Time Brachytherapy Catheter Positioning
- PMID: 28843373
- PMCID: PMC5720929
- DOI: 10.1016/j.ijrobp.2017.05.054
Prospective Clinical Implementation of a Novel Magnetic Resonance Tracking Device for Real-Time Brachytherapy Catheter Positioning
Abstract
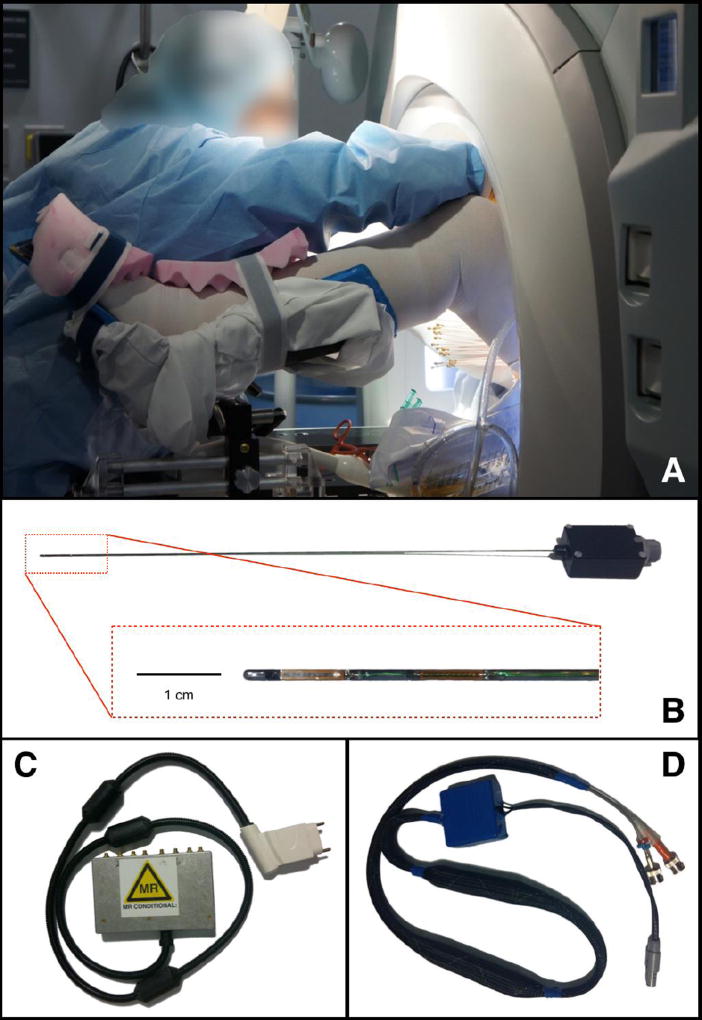
Purpose: We designed and built dedicated active magnetic resonance (MR)-tracked (MRTR) stylets. We explored the role of MRTR in a prospective clinical trial.
Methods and materials: Eleven gynecologic cancer patients underwent MRTR to rapidly optimize interstitial catheter placement. MRTR catheter tip location and orientation were computed and overlaid on images displayed on in-room monitors at rates of 6 to 16 frames per second. Three modes of actively tracked navigation were analyzed: coarse navigation to the approximate region around the tumor; fine-tuning, bringing the stylets to the desired location; and pullback, with MRTR stylets rapidly withdrawn from within the catheters, providing catheter trajectories for radiation treatment planning (RTP). Catheters with conventional stylets were inserted, forming baseline locations. MRTR stylets were substituted, and catheter navigation was performed by a clinician working inside the MRI bore, using monitor feedback.
Results: Coarse navigation allowed repositioning of the MRTR catheters tips by 16 mm (mean), relative to baseline, in 14 ± 5 s/catheter (mean ± standard deviation [SD]). The fine-tuning mode repositioned the catheter tips by a further 12 mm, in 24 ± 17 s/catheter. Pullback mode provided catheter trajectories with RTP point resolution of ∼1.5 mm, in 1 to 9 s/catheter.
Conclusions: MRTR-based navigation resulted in rapid and optimal placement of interstitial brachytherapy catheters. Catheters were repositioned compared with the initial insertion without tracking. In pullback mode, catheter trajectories matched computed tomographic precision, enabling their use for RTP.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures



References
-
- Devic S. MRI simulation for radiotherapy treatment planning. Med Phys. 2012 Nov;39(11):6701–11. - PubMed
-
- Dempsey J, et al. A Device For Realtime 3D Image-Guided IMRT. International Journal of Radiation Oncology Biology Physics. 2005;63:S202–S202.
-
- Viswanathan AN, Szymonifka J, Tempany-Afdhal CM, O'Farrell DA, Cormack RA. A prospective trial of real-time magnetic resonance-guided catheter placement in interstitial gynecologic brachytherapy. Brachytherapy. 2013 May-Jun;12(3):240–7. - PubMed
-
- Viswanathan AN, et al. Magnetic resonance-guided interstitial therapy for vaginal recurrence of endometrial cancer. Int J Radiat Oncol Biol Phys. 2006 Sep 1;66(1):91–9. - PubMed
-
- Damato AL, Viswanathan AN. Magnetic Resonance-Guided Gynecologic Brachytherapy. Magn Reson Imaging Clin N Am. 2015 Nov;23(4):633–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
