

Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for the Global Burden of Disease Study 2015
- PMID: 28843578
- PMCID: PMC5666185
- DOI: 10.1016/S1473-3099(17)30396-1
Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for the Global Burden of Disease Study 2015
Abstract
Background: The Global Burden of Diseases, Injuries, and Risk Factors (GBD) Study 2015 provides an up-to-date analysis of the burden of lower respiratory tract infections (LRIs) in 195 countries. This study assesses cases, deaths, and aetiologies spanning the past 25 years and shows how the burden of LRI has changed in people of all ages.
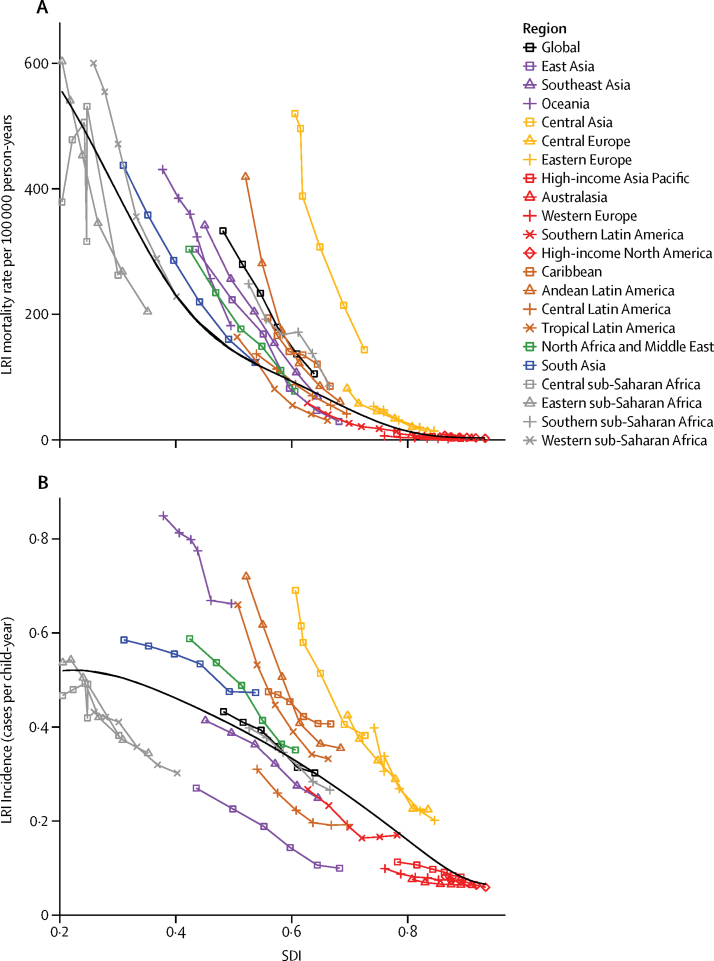
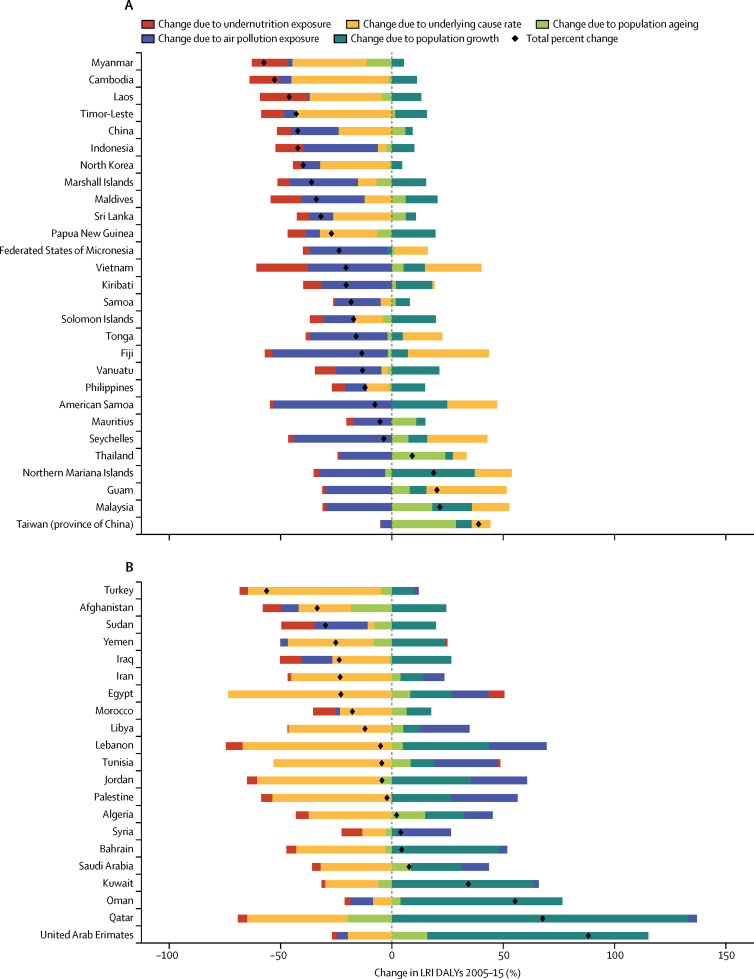
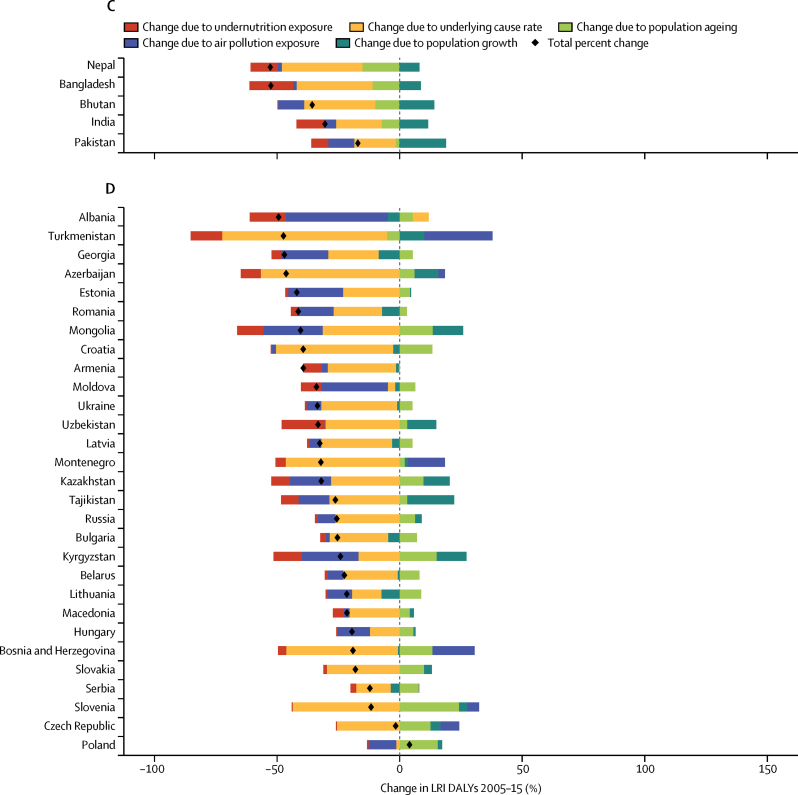
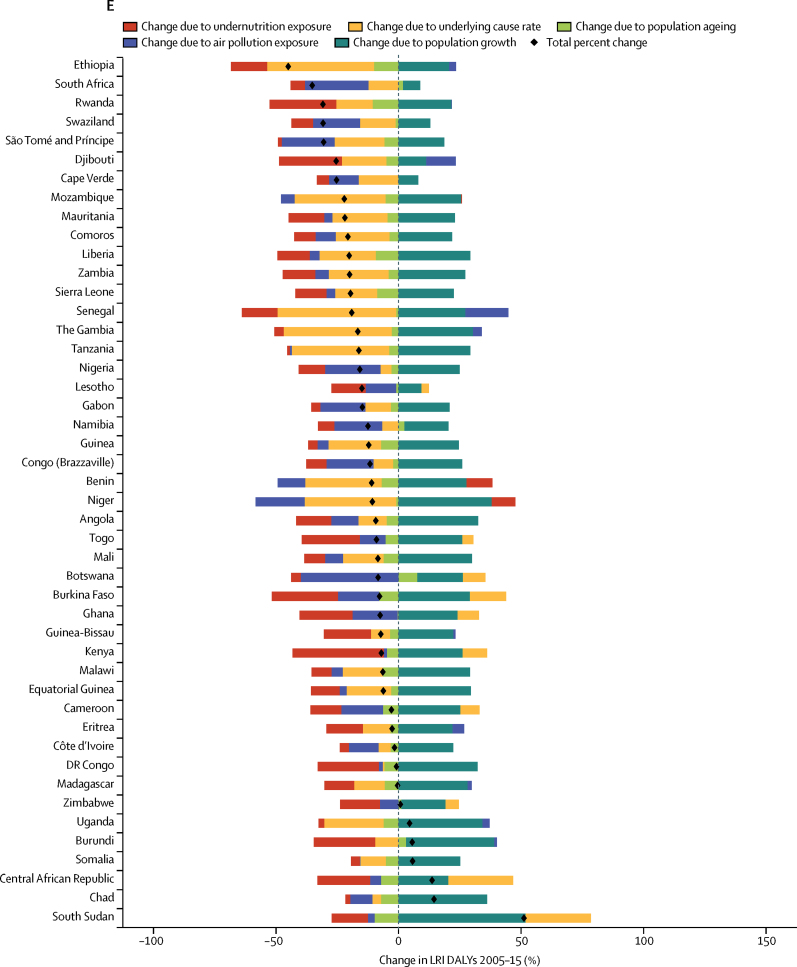
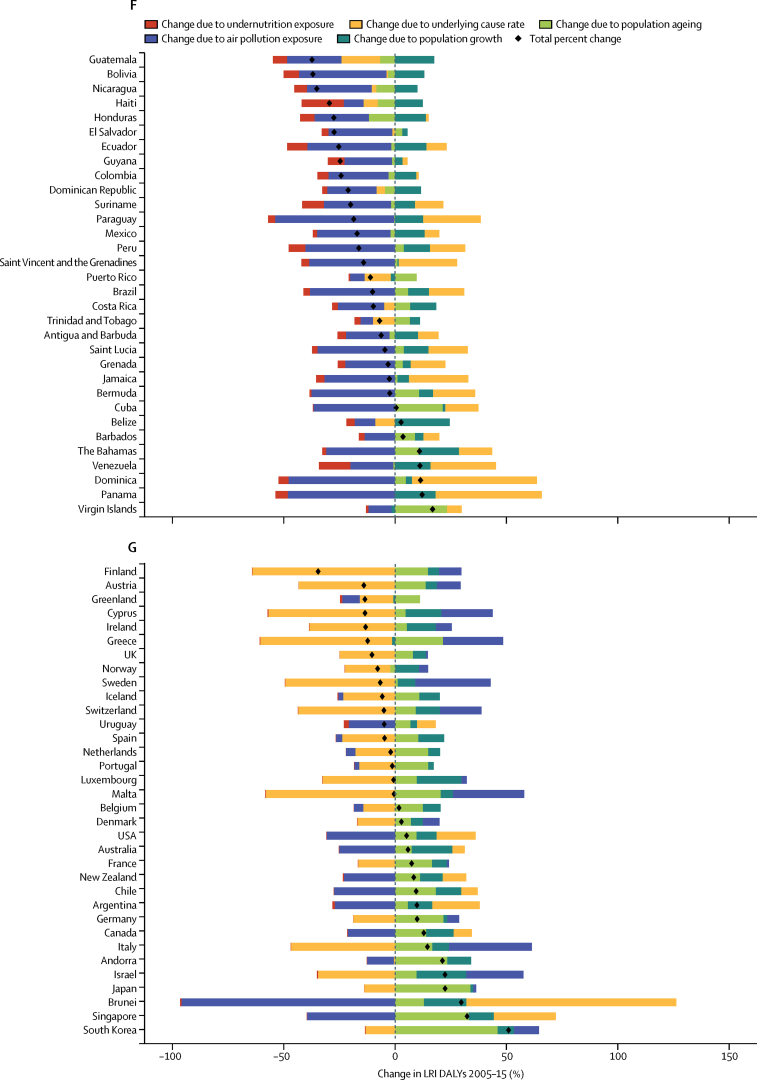
Methods: We estimated LRI mortality by age, sex, geography, and year using a modelling platform shared across most causes of death in the GBD 2015 study called the Cause of Death Ensemble model. We modelled LRI morbidity, including incidence and prevalence, using a meta-regression platform called DisMod-MR. We estimated aetiologies for LRI using two different counterfactual approaches, the first for viral pathogens, which incorporates the aetiology-specific risk of LRI and the prevalence of the aetiology in LRI episodes, and the second for bacterial pathogens, which uses a vaccine-probe approach. We used the Socio-demographic Index, which is a summary indicator derived from measures of income per capita, educational attainment, and fertility, to assess trends in LRI-related mortality. The two leading risk factors for LRI disability-adjusted life-years (DALYs), childhood undernutrition and air pollution, were used in a decomposition analysis to establish the relative contribution of changes in LRI DALYs.
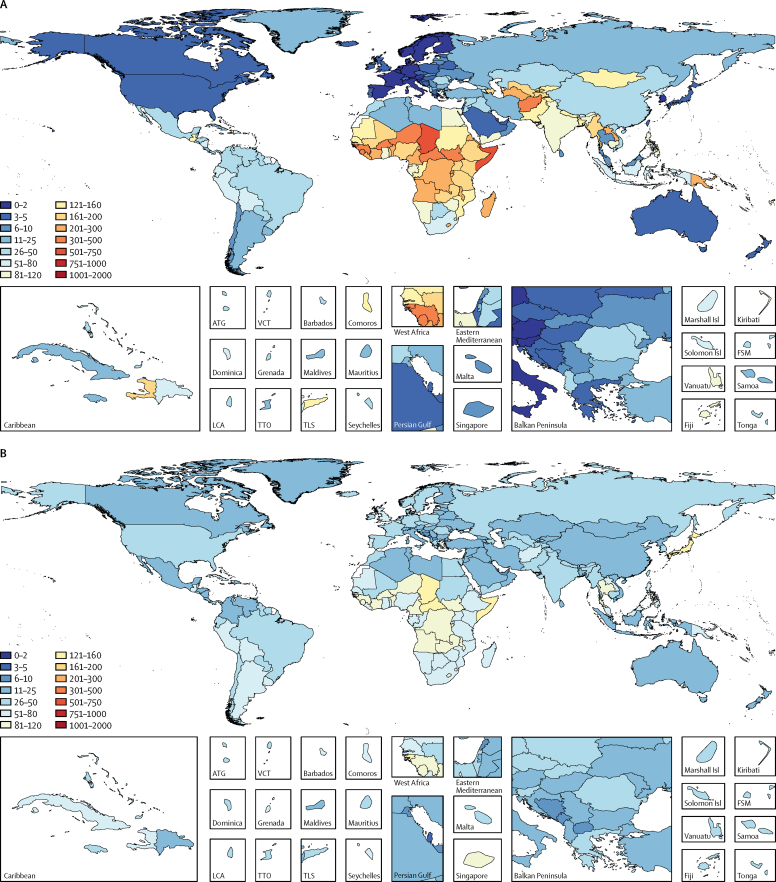
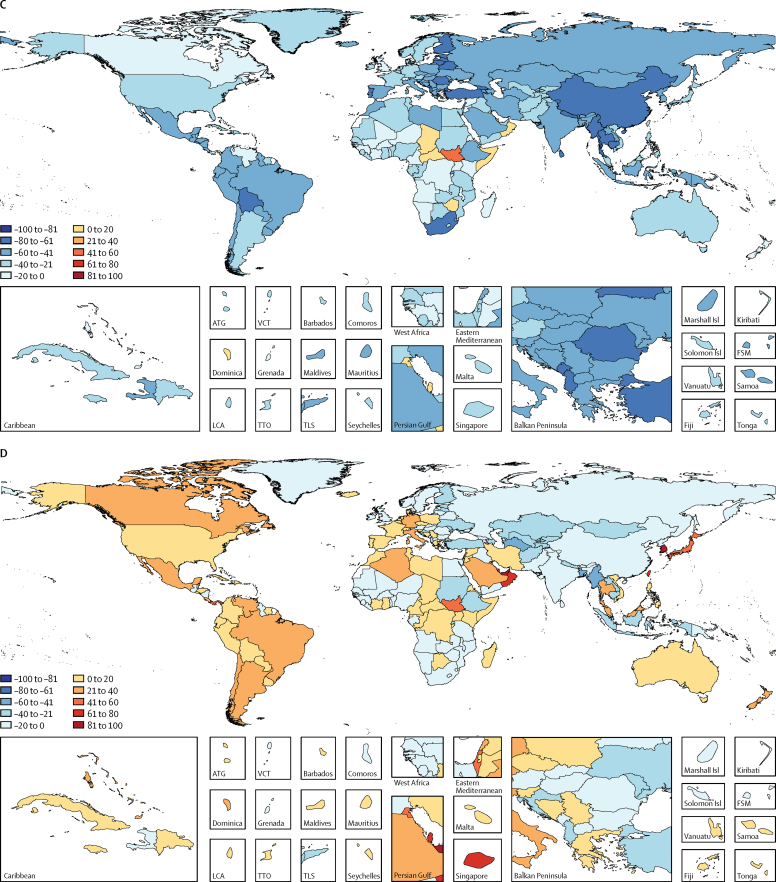
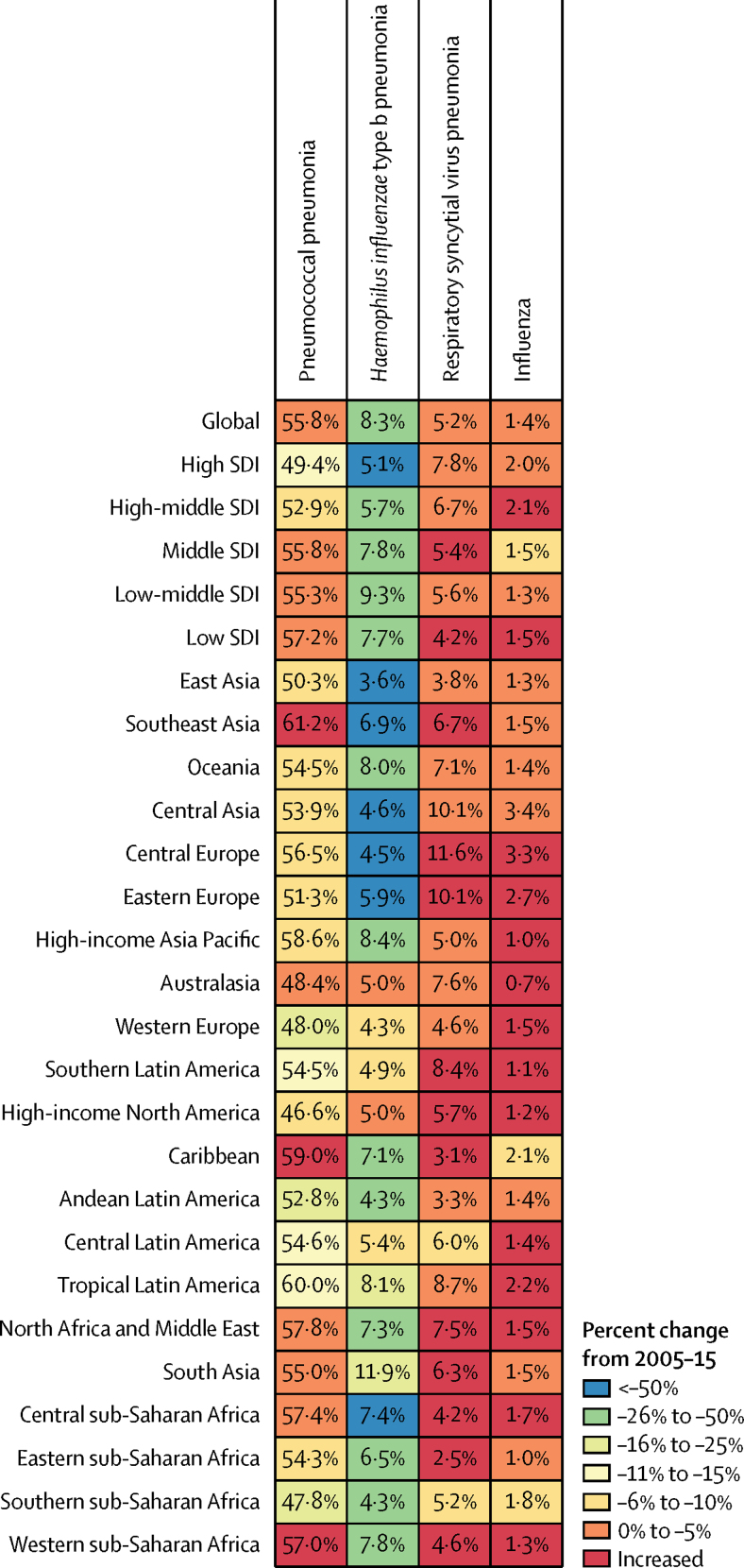
Findings: In 2015, we estimated that LRIs caused 2·74 million deaths (95% uncertainty interval [UI] 2·50 million to 2·86 million) and 103·0 million DALYs (95% UI 96·1 million to 109·1 million). LRIs have a disproportionate effect on children younger than 5 years, responsible for 704 000 deaths (95% UI 651 000-763 000) and 60.6 million DALYs (95ÙI 56·0-65·6). Between 2005 and 2015, the number of deaths due to LRI decreased by 36·9% (95% UI 31·6 to 42·0) in children younger than 5 years, and by 3·2% (95% UI -0·4 to 6·9) in all ages. Pneumococcal pneumonia caused 55·4% of LRI deaths in all ages, totalling 1 517 388 deaths (95% UI 857 940-2 183 791). Between 2005 and 2015, improvements in air pollution exposure were responsible for a 4·3% reduction in LRI DALYs and improvements in childhood undernutrition were responsible for an 8·9% reduction.
Interpretation: LRIs are the leading infectious cause of death and the fifth-leading cause of death overall; they are the second-leading cause of DALYs. At the global level, the burden of LRIs has decreased dramatically in the last 10 years in children younger than 5 years, although the burden in people older than 70 years has increased in many regions. LRI remains a largely preventable disease and cause of death, and continued efforts to decrease indoor and ambient air pollution, improve childhood nutrition, and scale up the use of the pneumococcal conjugate vaccine in children and adults will be essential in reducing the global burden of LRI.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Measuring progress on preventing pneumonia deaths: are we there yet?Lancet Infect Dis. 2017 Nov;17(11):1100-1101. doi: 10.1016/S1473-3099(17)30481-4. Epub 2017 Aug 23. Lancet Infect Dis. 2017. PMID: 28843577 No abstract available.
References
-
- Bhutta ZA, Das JK, Walker N. Interventions to address deaths from childhood pneumonia and diarrhoea equitably: what works and at what cost? Lancet. 2013;381:1417–1429. - PubMed
-
- UN Department of Economic and Social Affairs Sustainable Development Goal 3: ensure healthy lives and promote well-being for all at all ages. 2017. https://sustainabledevelopment.un.org/sdg3 (accessed Oct 10, 2016).
-
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1545–1602. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
