

Predictors of Use of Monitored Anesthesia Care for Outpatient Gastrointestinal Endoscopy in a Capitated Payment System
- PMID: 28843955
- PMCID: PMC5705328
- DOI: 10.1053/j.gastro.2017.08.030
Predictors of Use of Monitored Anesthesia Care for Outpatient Gastrointestinal Endoscopy in a Capitated Payment System
Abstract
Background & aims: Use of monitored anesthesia care (MAC) for gastrointestinal endoscopy has increased in the Veterans Health Administration (VHA) as in fee-for-service environments, despite the absence of financial incentives. We investigated factors associated with use of MAC in an integrated health care delivery system with a capitated payment model.
Methods: We performed a retrospective cohort study using multilevel logistic regression, with MAC use modeled as a function of procedure year, patient- and provider-level factors, and facility effects. We collected data from 2,091,590 veterans who underwent outpatient esophagogastroduodenoscopy and/or colonoscopy during fiscal years 2000-2013 at 133 facilities.
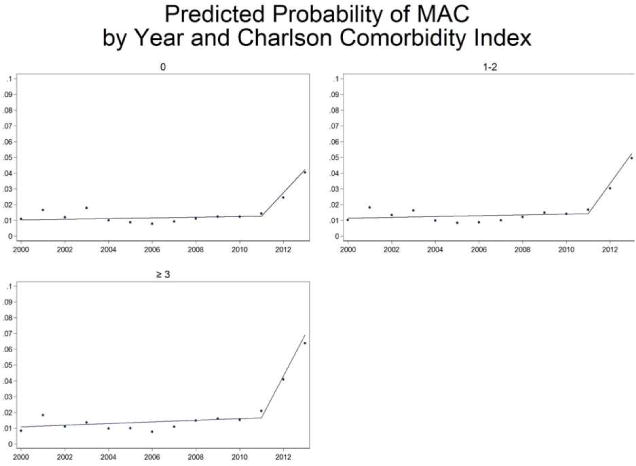
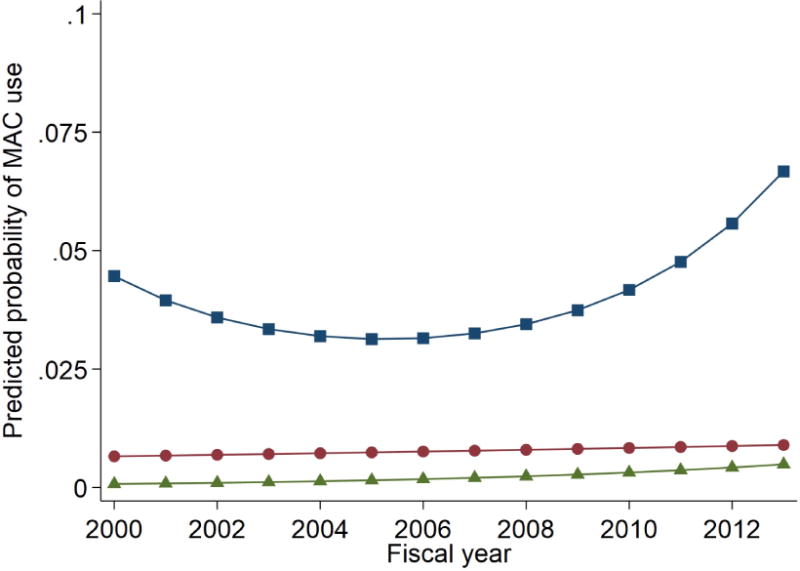
Results: The adjusted rate of MAC use in the VHA increased 17% per year (odds ratio for increase, 1.17; 95% confidence interval, 1.09-1.27) from fiscal year 2000 through 2013. The most rapid increase occurred starting in 2011. VHA use of MAC was associated with patient-level factors that included obesity, obstructive sleep apnea, higher comorbidity, and use of prescription opioids and/or benzodiazepines, although the magnitude of these effects was small. Provider-level and facility factors were also associated with use of MAC, although again the magnitude of these associations was small. Unmeasured facility-level effects had the greatest effect on the trend of MAC use.
Conclusions: In a retrospective study of veterans who underwent outpatient esophagogastroduodenoscopy and/or colonoscopy from fiscal year 2000 through 2013, we found that even in a capitated system, patient factors are only weakly associated with use of MAC. Facility-level effects are the most prominent factor influencing increasing use of MAC. Future studies should focus on better defining the role of MAC and facility and organizational factors that affect choice of endoscopic sedation. It will also be important to align resources and incentives to promote appropriate allocation of MAC based on clinically meaningful patient factors.
Keywords: Gastrointestinal Endoscopy; Monitored Anesthesia Care; Sedation; Veterans.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Centers for Medicare & Medicaid Services; US Department of Health and Human Services. Medicare program: revisions to payment policies under the Physician Fee Schedule and other revisions to Part B for CY 2017. Fed Regist. 2016;81(136):46162–46476.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
