

Active Surveillance Versus Watchful Waiting for Localized Prostate Cancer: A Model to Inform Decisions
- PMID: 28844371
- PMCID: PMC5694372
- DOI: 10.1016/j.eururo.2017.07.018
Active Surveillance Versus Watchful Waiting for Localized Prostate Cancer: A Model to Inform Decisions
Abstract
Background: An increasing proportion of prostate cancer is being managed conservatively. However, there are no randomized trials or consensus regarding the optimal follow-up strategy.
Objective: To compare life expectancy and quality of life between watchful waiting (WW) versus different strategies of active surveillance (AS).
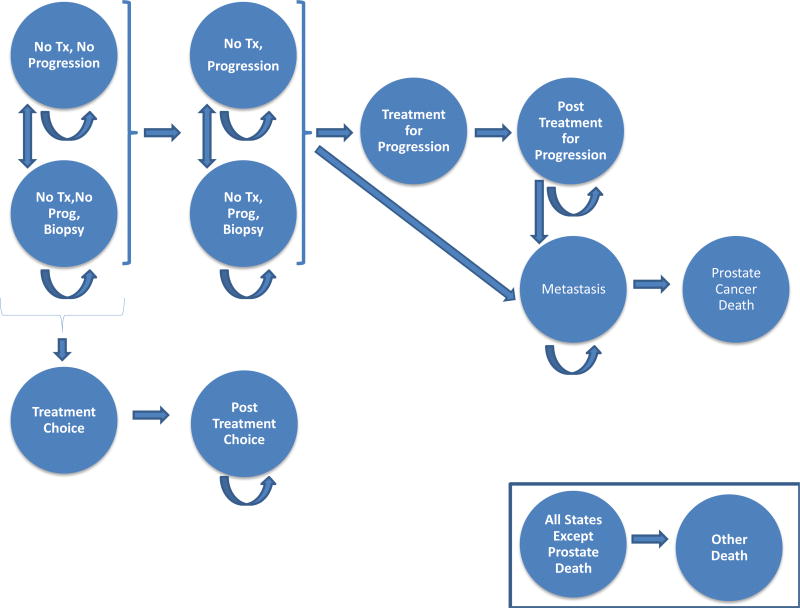
Design, setting, and participants: A Markov model was created for US men starting at age 50, diagnosed with localized prostate cancer who chose conservative management by WW or AS using different testing protocols (prostate-specific antigen every 3-6 mo, biopsy every 1-5 yr, or magnetic resonance imaging based). Transition probabilities and utilities were obtained from the literature.
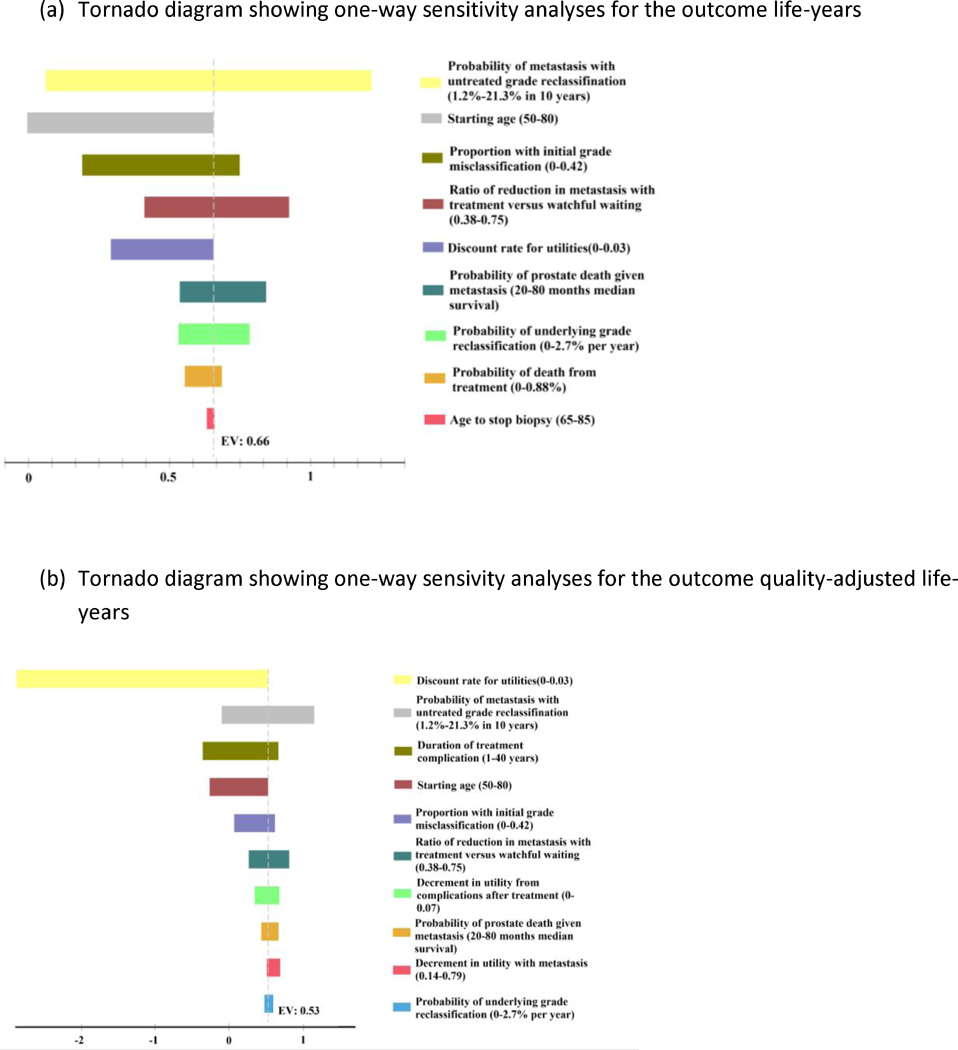
Outcome measurements and statistical analysis: Primary outcomes were life years and quality-adjusted life years (QALYs). Secondary outcomes include radical treatment, metastasis, and prostate cancer death.
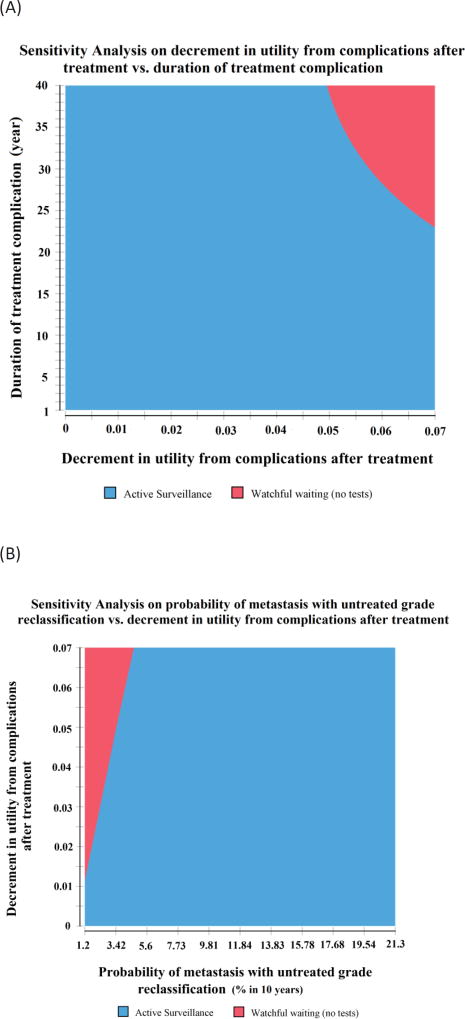
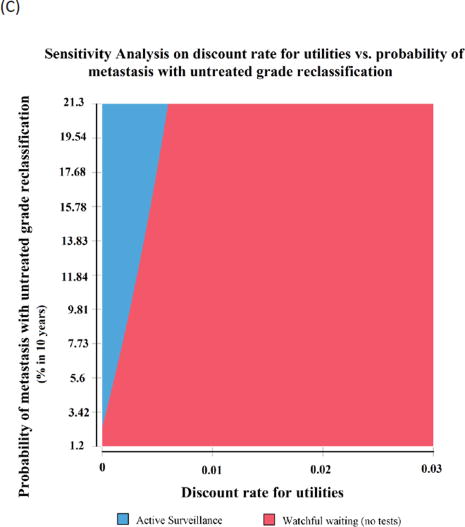
Results and limitations: All AS strategies yielded more life years compared with WW. Lifetime risks of prostate cancer death and metastasis were, respectively, 5.42% and 6.40% with AS versus 8.72% and 10.30% with WW. AS yielded more QALYs than WW except in cohorts age >65 yr at diagnosis, or when treatment-related complications were long term. The preferred follow-up strategy was also sensitive to whether people value short-term over long-term benefits (time preference). Depending on the AS protocol, 30-41% underwent radical treatment within 10 yr. Extending the surveillance biopsy interval from 1 to 5 yr reduced life years slightly, with a 0.26 difference in QALYs.
Conclusions: AS extends life more than WW, particularly for men with higher-risk features, but this is partly offset by the decrement in quality of life since many men eventually receive treatment.
Patient summary: More intensive active surveillance protocols extend life more than watchful waiting, but this is partly offset by decrements in quality of life from subsequent treatment.
Keywords: Active surveillance; Conservative management; Markov model; Prostate cancer; Watchful waiting.
Copyright © 2017 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Real-time Watchful Surveillance Looks Like Active Waiting.Eur Urol. 2017 Dec;72(6):908-909. doi: 10.1016/j.eururo.2017.08.003. Epub 2017 Aug 17. Eur Urol. 2017. PMID: 28822584 No abstract available.
References
-
- Barry MJ. Screening for prostate cancer--the controversy that refuses to die. N Engl J Med. 2009;360:1351–4. - PubMed
-
- Etzioni R, Penson DF, Legler JM, et al. Overdiagnosis due to prostate-specific antigen screening: lessons from U.S. prostate cancer incidence trends. J Natl Cancer Inst. 2002;94:981–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
