

All-cause mortality in young women with endometrial cancer receiving progesterone therapy
- PMID: 28844824
- PMCID: PMC5712259
- DOI: 10.1016/j.ajog.2017.08.007
All-cause mortality in young women with endometrial cancer receiving progesterone therapy
Abstract
Background: Uterine-preserving therapy with progesterone may be used in young women with endometrial cancer who desire fertility preservation. Such therapy delays definitive treatment with hysterectomy.
Objective: We examined the use and safety of progestational therapy in young women with endometrial cancer. The primary outcome of the analysis was overall survival.
Study design: We identified women ≤49 years of age with stage I endometrial cancer in the National Cancer Database from 2004 through 2014. Women treated with hormonal therapy with or without hysterectomy were compared to women treated with hysterectomy. After propensity score weighting, overall survival was examined using proportional hazards models.
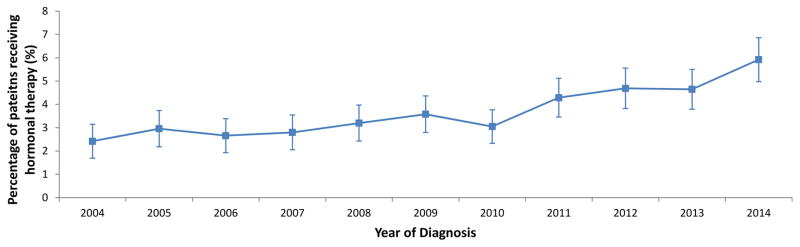
Results: A total of 23,231 patients, including 872 (3.8%) women treated with hormonal therapy were identified. Use of hormonal therapy was 2.4% (95% confidence interval, 1.8-3.3%) in 2004 and increased over time to 5.9% (95% confidence interval, 5.0-6.9%) by 2014 (P < .0001). Use of hormonal therapy decreased with older age, higher substage, and increasing grade. Black women were more likely to receive hormonal therapy while Medicaid recipients were less likely to receive hormonal therapy. The 5-year survival for patients treated with hormonal therapy was 96.4% (95% confidence interval, 94.3-98.0%) compared to 97.2% (95% confidence interval, 96.9-97.4%) for hysterectomy. In a multivariable model, women treated with hormonal therapy were 92% (hazard ratio, 1.92; 95% confidence interval, 1.15-3.19) more likely to die compared to women who underwent primary hysterectomy. When stratified by stage, hormonal therapy was associated with increased mortality in women with stage IB and I-not otherwise specified tumors but not for stage IA neoplasms.
Conclusion: Use of progestational therapy is increasing. Its use was associated with decreased survival, particularly in women with stage IB tumors.
Keywords: endometrial cancer; progesterone; uterine cancer.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest or disclosures.
Figures
Comment in
-
Reply.Am J Obstet Gynecol. 2018 Mar;218(3):363-364. doi: 10.1016/j.ajog.2017.11.584. Epub 2017 Nov 23. Am J Obstet Gynecol. 2018. PMID: 29175246 No abstract available.
-
Progesterone therapy in endometrial cancer.Am J Obstet Gynecol. 2018 Mar;218(3):362-363. doi: 10.1016/j.ajog.2017.11.583. Epub 2017 Nov 23. Am J Obstet Gynecol. 2018. PMID: 29175256 No abstract available.
-
All-cause death in young women with endometrial cancer who receive progesterone therapy.Am J Obstet Gynecol. 2018 Jul;219(1):119. doi: 10.1016/j.ajog.2018.03.009. Epub 2018 Mar 9. Am J Obstet Gynecol. 2018. PMID: 29530674 No abstract available.
-
Reply.Am J Obstet Gynecol. 2018 Jul;219(1):119-120. doi: 10.1016/j.ajog.2018.03.008. Epub 2018 Mar 9. Am J Obstet Gynecol. 2018. PMID: 29530676 No abstract available.
References
-
- Wright JD, Barrena Medel NI, Sehouli J, Fujiwara K, Herzog TJ. Contemporary management of endometrial cancer. Lancet. 2012;379:1352–60. - PubMed
-
- Wright JD, Buck AM, Shah M, Burke WM, Schiff PB, Herzog TJ. Safety of ovarian preservation in premenopausal women with endometrial cancer. J Clin Oncol. 2009;27:1214–9. - PubMed
-
- Shah MM, Wright JD. Management of endometrial cancer in young women. Clin Obstet Gynecol. 2011;54:219–25. - PubMed
-
- Gallos ID, Yap J, Rajkhowa M, Luesley DM, Coomarasamy A, Gupta JK. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: a systematic review and metaanalysis. Am J Obstet Gynecol. 2012;207:266, e1–12. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
