

Management of Adolescent Gynecomastia: An Update
- PMID: 28845839
- PMCID: PMC6166145
- DOI: 10.23750/abm.v88i2.6665
Management of Adolescent Gynecomastia: An Update
Abstract
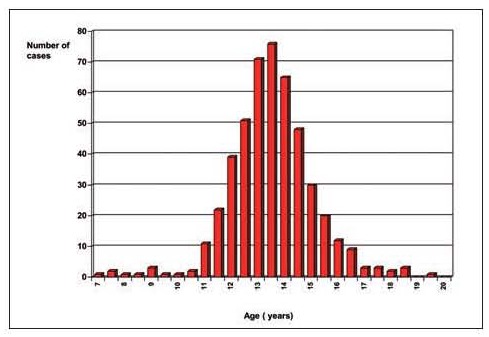
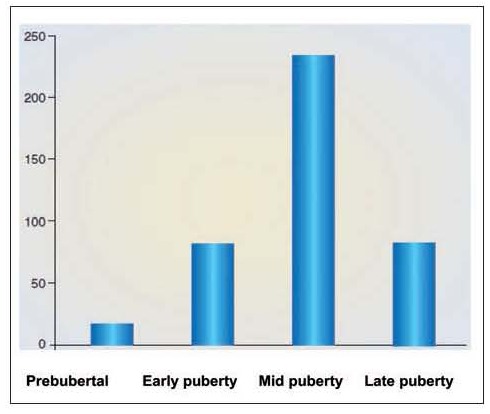
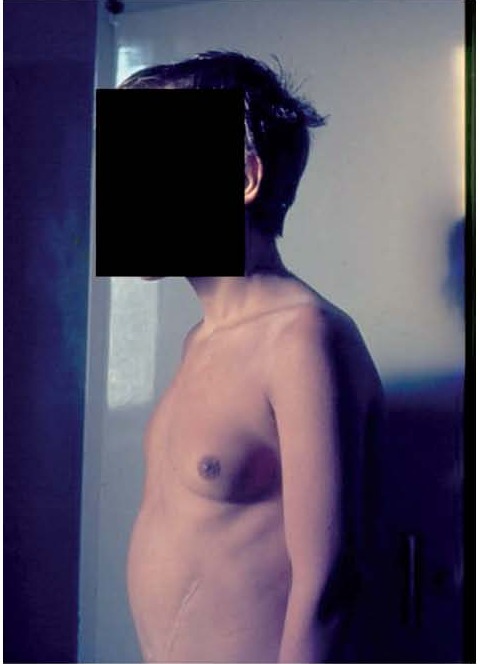
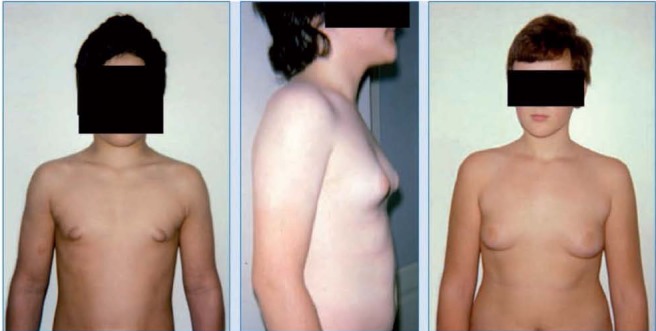
Gynecomastia refers to an enlargement of the male breast caused by benign proliferation of the glands ducts and stromal components including fat. It is the most common form of breast swelling seen in adolescent males. During pubertal development, gynecomastia can develop as a result of transient relative imbalances between androgens and estrogens. Pubertal gynecomastia is self-limited in 75 to 90% of adolescents and regresses over 1 to 3 years. However it may cause significant psychological stress and depression in adolescents. For boys with persistent gynecomastia that is causing substantial tenderness or embarrassment a tailored approach of close follow-up and use of anti-estrogen drugs may be recommended. These drugs block the effects of estrogens in the body and can reduce the size of the breasts somewhat. It appears that pharmacological therapy of persistent adolescent gynecomastia is reasonable effective if given early in the course of the disease and more successful in cases with small or moderate breast enlargement. However, neither of these drugs is universally approved for the treatment of gynecomastia because the risks and benefits have not been studied completely. Surgical approach may be needed under special conditions for cosmetic reasons. In this update, we review the different published trials for managing adolescent gynecomastia.
Keywords: gynecomastia, adolescents, androgens, estrogens, anti-estrogen drugs, mammary adenectomy, liposuction.
Figures

References
-
- Nuttall FQ. Gynecomastia as a physical finding in normal men. J Clin Endocrinol Metab. 1979;48:338–340. - PubMed
-
- Nydick M, Bustos J, Dale JH Jr, Rawson RW. Gynecomastia in adolescent boys. JAMA. 1961;178:449–454. - PubMed
-
- Ma NS, Geffner ME. Gynecomastia in prepubertal and pubertal men. Curr Opin Pediatr. 2008;20:465–470. - PubMed
-
- Bembo SA, Carlson HE. Gynecomastia: its features, and when and how to treat it. Cleve Clin J Med. 2004;71:511–517. - PubMed
-
- Braunstein GD. Gynecomastia. N Engl J Med. 1993;328:490–495. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources