

Association of Genetic Variants Related to CETP Inhibitors and Statins With Lipoprotein Levels and Cardiovascular Risk
- PMID: 28846118
- PMCID: PMC5710502
- DOI: 10.1001/jama.2017.11467
Association of Genetic Variants Related to CETP Inhibitors and Statins With Lipoprotein Levels and Cardiovascular Risk
Abstract
Importance: Some cholesteryl ester transfer protein (CETP) inhibitors lower low-density lipoprotein cholesterol (LDL-C) levels without reducing cardiovascular events, suggesting that the clinical benefit of lowering LDL-C may depend on how LDL-C is lowered.
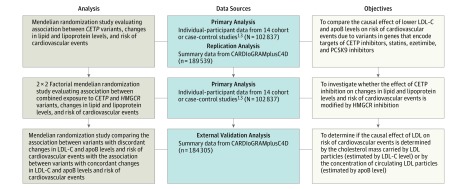
Objective: To estimate the association between changes in levels of LDL-C (and other lipoproteins) and the risk of cardiovascular events related to variants in the CETP gene, both alone and in combination with variants in the 3-hydroxy-3-methylglutaryl-CoA reductase (HMGCR) gene.
Design, setting, and participants: Mendelian randomization analyses evaluating the association between CETP and HMGCR scores, changes in lipid and lipoprotein levels, and the risk of cardiovascular events involving 102 837 participants from 14 cohort or case-control studies conducted in North America or the United Kingdom between 1948 and 2012. The associations with cardiovascular events were externally validated in 189 539 participants from 48 studies conducted between 2011 and 2015.
Exposures: Differences in mean high-density lipoprotein cholesterol (HDL-C), LDL-C, and apolipoprotein B (apoB) levels in participants with CETP scores at or above vs below the median.
Main outcomes and measures: Odds ratio (OR) for major cardiovascular events.
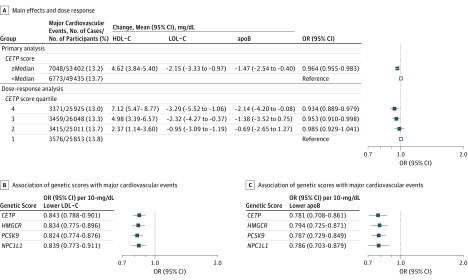
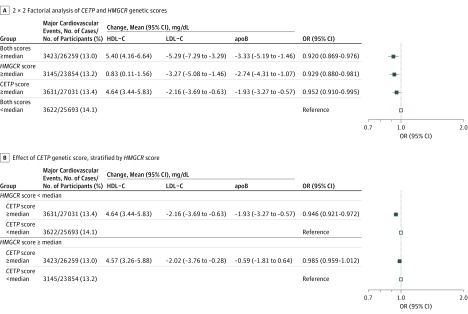
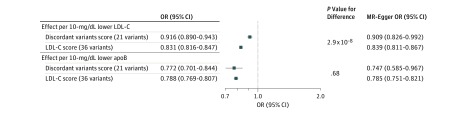
Results: The primary analysis included 102 837 participants (mean age, 59.9 years; 58% women) who experienced 13 821 major cardiovascular events. The validation analyses included 189 539 participants (mean age, 58.5 years; 39% women) with 62 240 cases of coronary heart disease (CHD). Considered alone, the CETP score was associated with higher levels of HDL-C, lower LDL-C, concordantly lower apoB, and a corresponding lower risk of major vascular events (OR, 0.946 [95% CI, 0.921-0.972]) that was similar in magnitude to the association between the HMGCR score and risk of major cardiovascular events per unit change in levels of LDL-C (and apoB). When combined with the HMGCR score, the CETP score was associated with the same reduction in LDL-C levels but an attenuated reduction in apoB levels and a corresponding attenuated nonsignificant risk of major cardiovascular events (OR, 0.985 [95% CI, 0.955-1.015]). In external validation analyses, a genetic score consisting of variants with naturally occurring discordance between levels of LDL-C and apoB was associated with a similar risk of CHD per unit change in apoB level (OR, 0.782 [95% CI, 0.720-0.845] vs 0.793 [95% CI, 0.774-0.812]; P = .79 for difference), but a significantly attenuated risk of CHD per unit change in LDL-C level (OR, 0.916 [95% CI, 0.890-0.943] vs 0.831 [95% CI, 0.816-0.847]; P < .001) compared with a genetic score associated with concordant changes in levels of LDL-C and apoB.
Conclusions and relevance: Combined exposure to variants in the genes that encode the targets of CETP inhibitors and statins was associated with discordant reductions in LDL-C and apoB levels and a corresponding risk of cardiovascular events that was proportional to the attenuated reduction in apoB but significantly less than expected per unit change in LDL-C. The clinical benefit of lowering LDL-C levels may therefore depend on the corresponding reduction in apoB-containing lipoprotein particles.
Conflict of interest statement
Figures
Comment in
-
Genetic Studies Help Clarify the Complexities of Lipid Biology and Treatment.JAMA. 2017 Sep 12;318(10):915-917. doi: 10.1001/jama.2017.11750. JAMA. 2017. PMID: 28846117 No abstract available.
References
-
- Ference BA, Yoo W, Alesh I, et al. . Effect of long-term exposure to lower low-density lipoprotein cholesterol beginning early in life on the risk of coronary heart disease. J Am Coll Cardiol. 2012;60(25):2631-2639. - PubMed
-
- Silverman MG, Ference BA, Im K, et al. . Association between lowering LDL-C and cardiovascular risk reduction among different therapeutic interventions: a systematic review and meta-analysis. JAMA. 2016;316(12):1289-1297. - PubMed
-
- Ference BA, Ginsberg HN, Graham I, et al. . Low-density lipoproteins cause atherosclerotic cardiovascular disease, 1: evidence from genetic, epidemiologic and clinical studies: a consensus statement from the European Atherosclerosis Society Consensus Panel [published online April 24, 2017]. Eur Heart J. doi:10.1093/eurheartj/ehx144 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
