

Do Less Harm: Evaluating HIV Programmatic Alternatives in Response to Cutbacks in Foreign Aid
- PMID: 28847013
- PMCID: PMC5675810
- DOI: 10.7326/M17-1358
Do Less Harm: Evaluating HIV Programmatic Alternatives in Response to Cutbacks in Foreign Aid
Abstract
Background: Resource-limited nations must consider their response to potential contractions in international support for HIV programs.
Objective: To evaluate the clinical, epidemiologic, and budgetary consequences of alternative HIV program scale-back strategies in 2 recipient nations, the Republic of South Africa (RSA) and Côte d'Ivoire (CI).
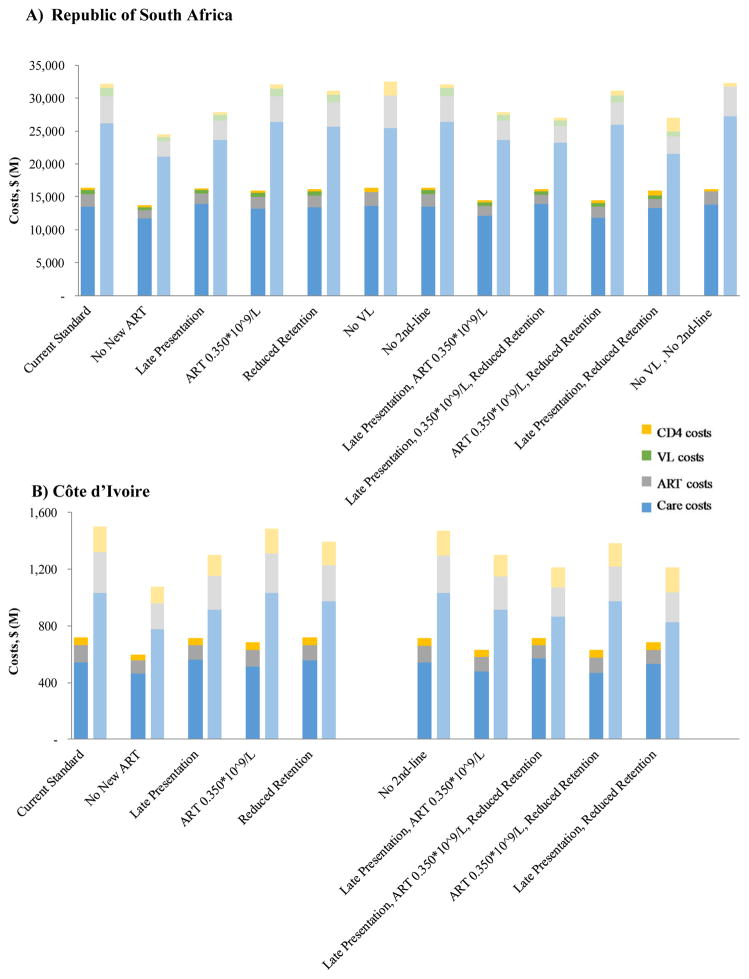
Design: Model-based comparison between current standard (CD4 count at presentation of 0.260 × 109 cells/L, universal antiretroviral therapy [ART] eligibility, and 5-year retention rate of 84%) and scale-back alternatives, including reduced HIV detection, no ART or delayed initiation (when CD4 count is <0.350 × 109 cells/L), reduced investment in retention, and no viral load monitoring or second-line ART.
Data sources: Published RSA- and CI-specific estimates of the HIV care continuum, ART efficacy, and HIV-related costs.
Target population: HIV-infected persons, including future incident cases.
Time horizon: 5 and 10 years.
Perspective: Modified societal perspective, excluding time and productivity costs.
Outcome measures: HIV transmissions and deaths, years of life, and budgetary outlays (2015 U.S. dollars).
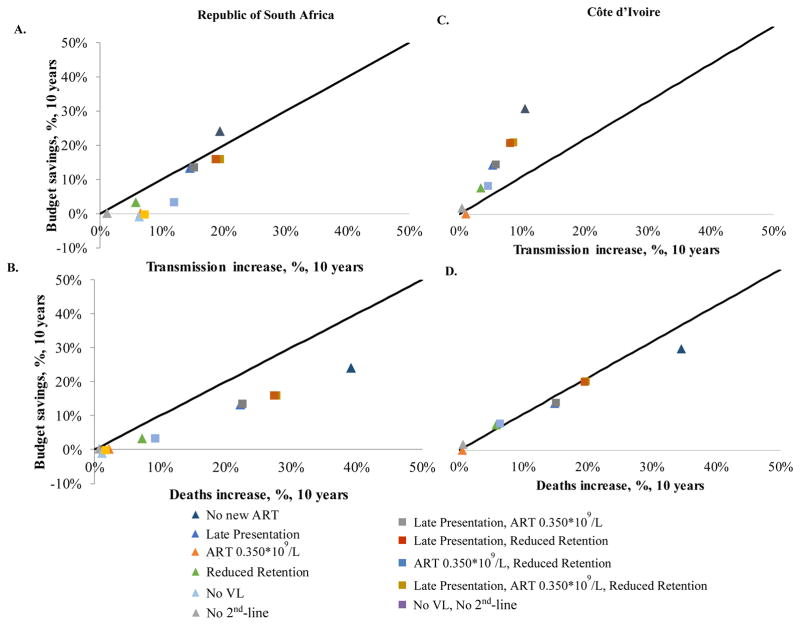
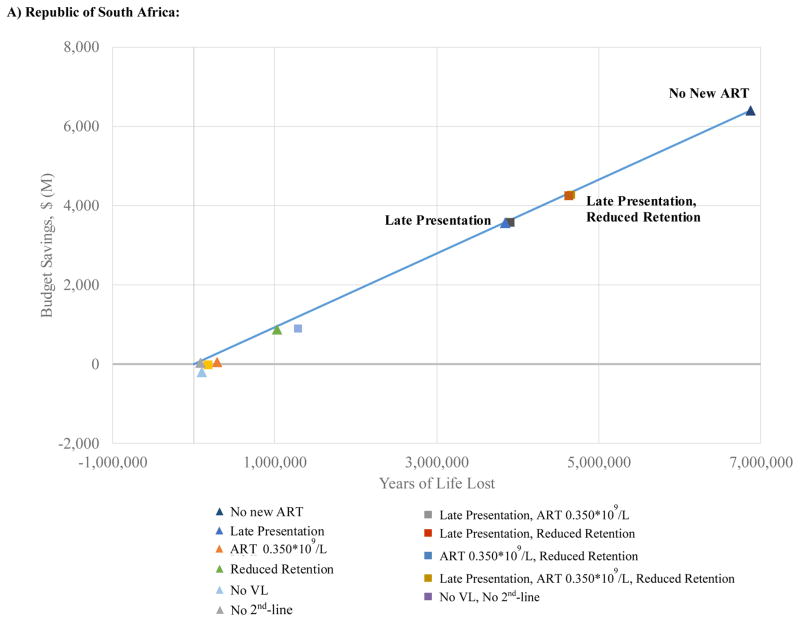
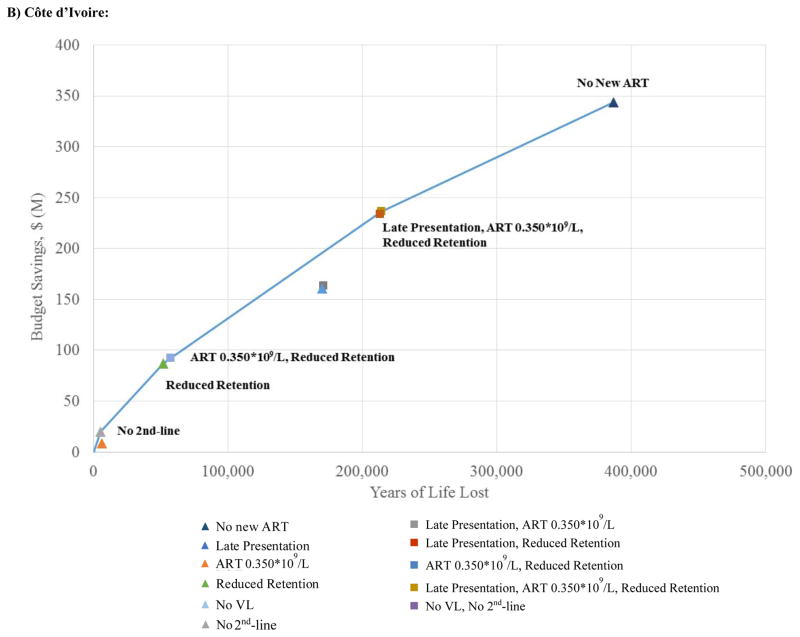
Results of base-case analysis: At 10 years, scale-back strategies increase projected HIV transmissions by 0.5% to 19.4% and deaths by 0.6% to 39.1%. Strategies can produce budgetary savings of up to 30% but no more. Compared with the current standard, nearly every scale-back strategy produces proportionally more HIV deaths (and transmissions, in RSA) than savings. When the least harmful and most efficient alternatives for achieving budget cuts of 10% to 20% are applied, every year of life lost will save roughly $900 in HIV-related outlays in RSA and $600 to $900 in CI.
Results of sensitivity analysis: Scale-back programs, when combined, may result in clinical and budgetary synergies and offsets.
Limitation: The magnitude and details of budget cuts are not yet known, nor is the degree to which other international partners might step in to restore budget shortfalls.
Conclusion: Scaling back international aid to HIV programs will have severe adverse clinical consequences; for similar economic savings, certain programmatic scale-back choices result in less harm than others.
Primary funding source: National Institutes of Health and Steve and Deborah Gorlin MGH Research Scholars Award.
Figures
References
-
- 90-90-90: an ambitious treatment target to help end the AIDS epidemic. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2014. [Accessed 14 July 2017]. at http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf.
-
- Williams BG, Gupta S, Wollmers M, Granich R. The impact and cost of ending AIDS in Botswana. Lancet HIV. 2016;3(9):e409. - PubMed
-
- Daschle T, Frist B. The case for strategic health diplomacy: a study of PEPFAR. Washington, DC: Bipartisan Policy Center; 2015. [Accessed 12 July 2017]. at http://cdn.bipartisanpolicy.org/wp-content/uploads/2015/11/BPC_Strategic....
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials