

Perinatal suicide in Ontario, Canada: a 15-year population-based study
- PMID: 28847780
- PMCID: PMC5573543
- DOI: 10.1503/cmaj.170088
Perinatal suicide in Ontario, Canada: a 15-year population-based study
Abstract
Background: Death by suicide during the perinatal period has been understudied in Canada. We examined the epidemiology of and health service use related to suicides during pregnancy and the first postpartum year.
Methods: In this retrospective, population-based cohort study, we linked health administrative databases with coroner death records (1994-2008) for Ontario, Canada. We compared sociodemographic characteristics, clinical features and health service use in the 30 days and 1 year before death between women who died by suicide perinatally, women who died by suicide outside of the perinatal period and living perinatal women.
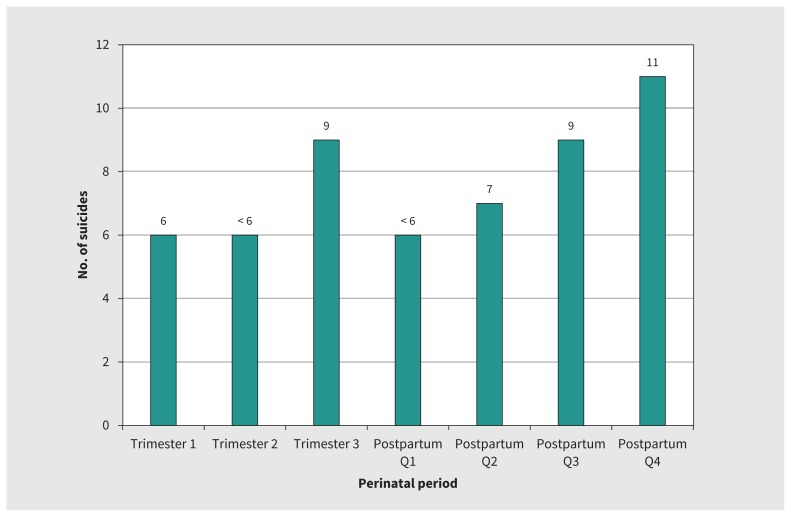
Results: The perinatal suicide rate was 2.58 per 100 000 live births, with suicide accounting for 51 (5.3%) of 966 perinatal deaths. Most suicides occurred during the final quarter of the first postpartum year, with highest rates in rural and remote regions. Perinatal women were more likely to die from hanging (33.3% [17/51]) or jumping or falling (19.6% [10/51]) than women who died by suicide non-perinatally (p = 0.04). Only 39.2% (20/51) had mental health contact within the 30 days before death, similar to the rate among those who died by suicide non-perinatally (47.7% [762/1597]; odds ratio [OR] 0.71, 95% confidence interval [CI] 0.40-1.25). Compared with living perinatal women matched by pregnancy or postpartum status at date of suicide, perinatal women who died by suicide had similar likelihood of non-mental health primary care and obstetric care before the index date but had a lower likelihood of pediatric contact (64.5% [20/31] v. 88.4% [137/155] at 30 days; OR 0.24, 95% CI 0.10-0.58).
Interpretation: The perinatal suicide rate for Ontario during the period 1994-2008 was comparable to international estimates and represents a substantial component of Canadian perinatal mortality. Given that deaths by suicide occur throughout the perinatal period, all health care providers must be collectively vigilant in assessing risk.
© 2017 Canadian Medical Association or its licensors.
Conflict of interest statement
Competing interests: Sophie Grigoriadis has received personal fees from Sage, Eli Lilly Canada, Allergan/Actavis, Pfizer and Bristol Myers Squibb for activities unrelated to the current manuscript. No other competing interests were declared.
Figures
Comment in
-
Could changes in pharmacotherapy peripregnancy contribute to the shift in means of suicide?CMAJ. 2017 Dec 4;189(48):E1497. doi: 10.1503/cmaj.733427. CMAJ. 2017. PMID: 29203620 Free PMC article. No abstract available.
-
Mental health care and suicide in pregnancy and postpartum.CMAJ. 2017 Dec 4;189(48):E1498. doi: 10.1503/cmaj.733429. CMAJ. 2017. PMID: 29203621 Free PMC article. No abstract available.
-
Peripartum suicide: additional considerations.CMAJ. 2018 Jan 15;190(2):E57. doi: 10.1503/cmaj.733569. CMAJ. 2018. PMID: 29335267 Free PMC article. No abstract available.
References
-
- Oates M. Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. Br Med Bull 2003;67:219–29. - PubMed
-
- Oates M. Suicide: the leading cause of maternal death. Br J Psychiatry 2003; 183:279–81. - PubMed
-
- Lewis G, editor. Saving mothers’ lives: reviewing maternal deaths to make motherhood safer — 2003–2005. Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London (UK): The Confidential Enquiry into Maternal and Child Health; 2007.
-
- Austin MP, Kildea S, Sullivan E. Maternal mortality and psychiatric morbidity in the perinatal period: challenges and opportunities for prevention in the Australian setting. Med J Aust 2007;186:364–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical