

Risk of Death by Comorbidity Prompting Rehospitalization Following the Initial COPD Hospitalization
- PMID: 28848828
- PMCID: PMC5556770
- DOI: 10.15326/jcopdf.2.1.2014.0129
Risk of Death by Comorbidity Prompting Rehospitalization Following the Initial COPD Hospitalization
Abstract
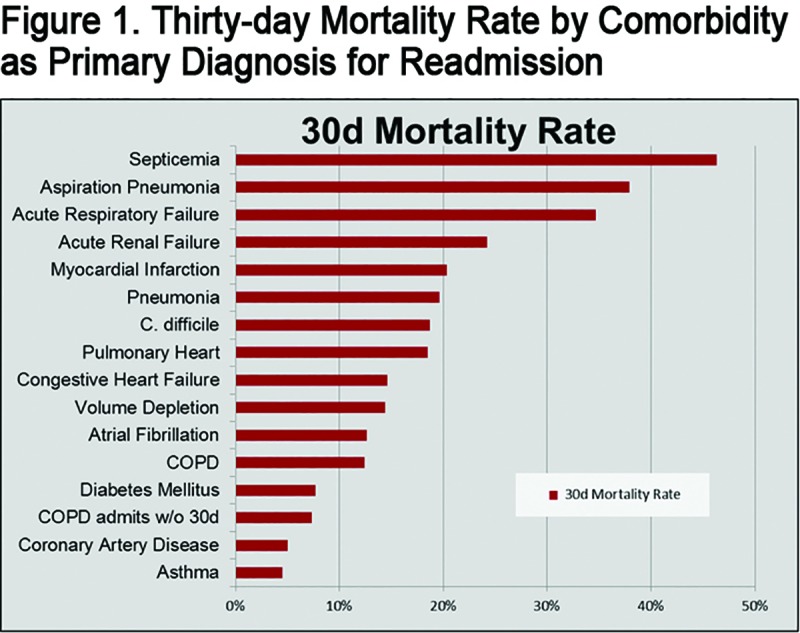
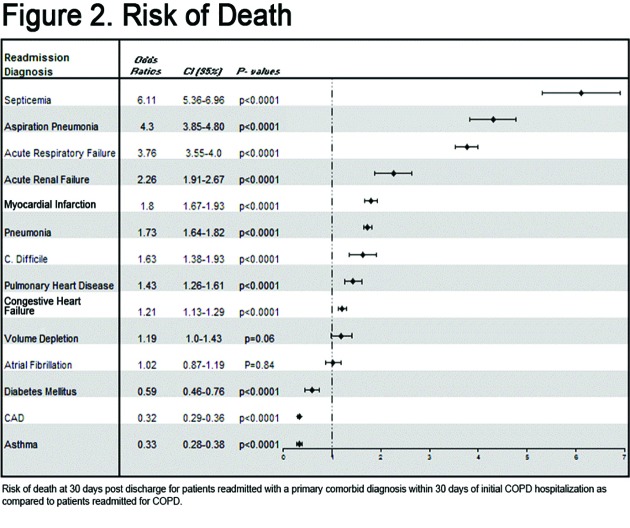
Rationale: Chronic obstructive pulmonary disease (COPD) hospitalizations increase short and long-term mortality; multiple COPD hospitalizations track with even higher mortality. While comorbidities such as coronary artery disease (CAD) and congestive heart failure (CHF) are common in COPD, their contribution to mortality risk after a sentinel COPD hospitalization is unknown. Purpose: Assess the effect on mortality of comorbid conditions prompting rehospitalization following COPD exacerbation hospitalization. Methods: We performed a retrospective cohort analysis of patients hospitalized for COPD exacerbations in Pennsylvania from 1990-2010 using the Pennsylvania Health Care Cost Containment Council (PHC4) database. We included patients > 40 years old hospitalized for an acute exacerbation of COPD (AECOPD; International Classification of Diseases-Ninth Edition, [ICD-9] #491, 492, 496) by discharge diagnosis. Thirty-day mortality in patients with COPD hospitalization for acute exacerbation who were rehospitalized for COPD < 30days post-discharge was compared to those primarily readmitted for comorbid conditions. Relative risk of death after readmission was determined by diagnosis. Primary end-point was mortality 30 days post-readmission for 14 most common non-COPD diagnoses, including heart failure, pneumonia, pulmonary embolus (PE), and myocardial infarction. Results: Patients were nearly 2 times more likely to die within 30 days when readmitted for pneumonia (p<0.0001) or myocardial infarction (p<0.0001) rather than COPD. Septicemia conferred the highest mortality. Conclusions: COPD patients rehospitalized for comorbid conditions such as myocardial infarction, pneumonia, septicemia or pulmonary heart disease (includes PE) were significantly more likely to die within 30 days than patients readmitted for COPD. Great emphasis is already placed on preventing COPD rehospitalization; however, more attention should focus on preemptive risk reduction for comorbidities in COPD patients.
Keywords: comorbidity; copd; hospitalization.
References
-
- Mannino DM. COPD epidemiology, prevalence, morbidity and mortality and disease heterogeneity. Chest. 2002;121(5Suppl):121S-126S. doi: http://dx.doi.org/10.1378/chest.121.5_suppl.121S - PubMed
-
- Mapel DW,Hurley JS,Frost FJ,Petersen HV,Picchi MA,Coultas DB. Health care utilization in chronic obstructive pulmonary disease. A case-control study in a health maintenance organization. Arch Intern Med. 2000;160(17):2653-2658. doi: http://dx.doi.org/10.1001/archinte.160.17.2653 - PubMed
-
- Mannino DM,Buist AS. Global burden of COPD: risk factor, prevalence, and future trends. Lancet. 2007;370(9589):765-773. doi: http://dx.doi.org/10.1016/S0140-6736(07)61380-4 - PubMed
-
- Hansell AL,Walk JA,Soriano JB. What do chronic obstructive pulmonary disease patients die from? A multiple cause coding analysis. Eur Respir J. 2003;22(5):809-814. doi: http://dx.doi.org/10.1183/09031936.03.00031403 - PubMed
-
- Mannino DM,Thorn D,Swensen A,Holguin F. Prevalence and outcomes of diabetes hypertension, and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962-969. doi: http://dx.doi.org/10.1183/09031936.00012408 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous