

The frequency and prognostic effect of TERT promoter mutation in diffuse gliomas
- PMID: 28851427
- PMCID: PMC5574236
- DOI: 10.1186/s40478-017-0465-1
The frequency and prognostic effect of TERT promoter mutation in diffuse gliomas
Abstract
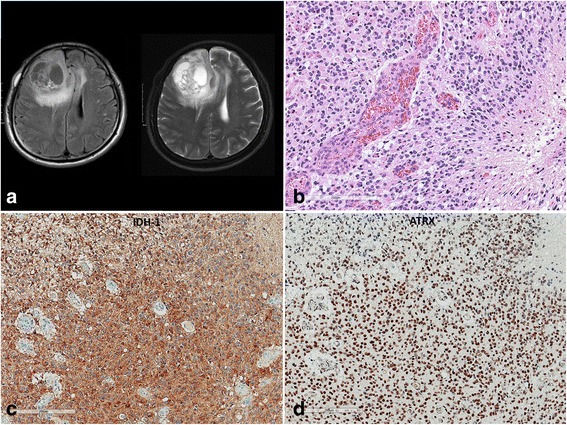
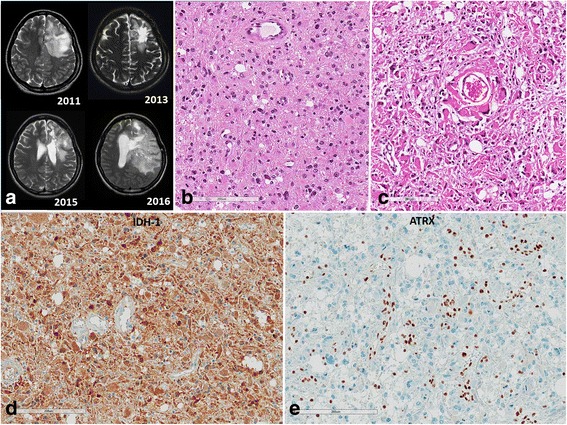
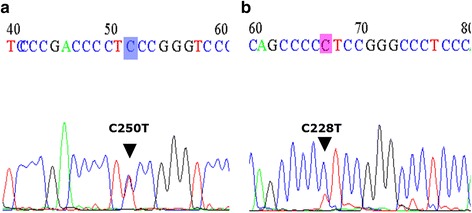
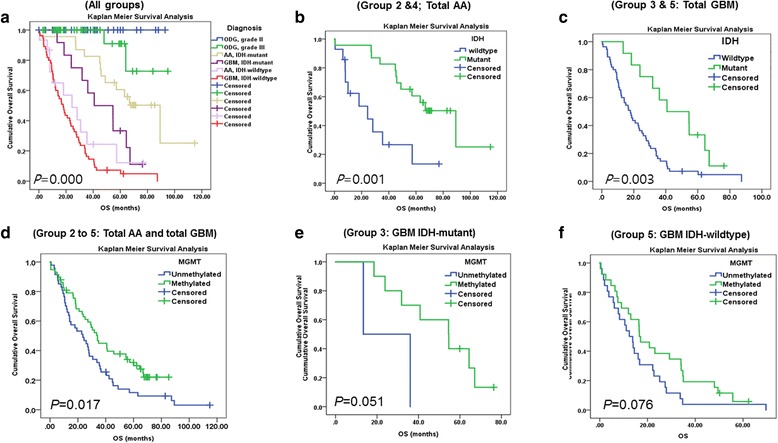
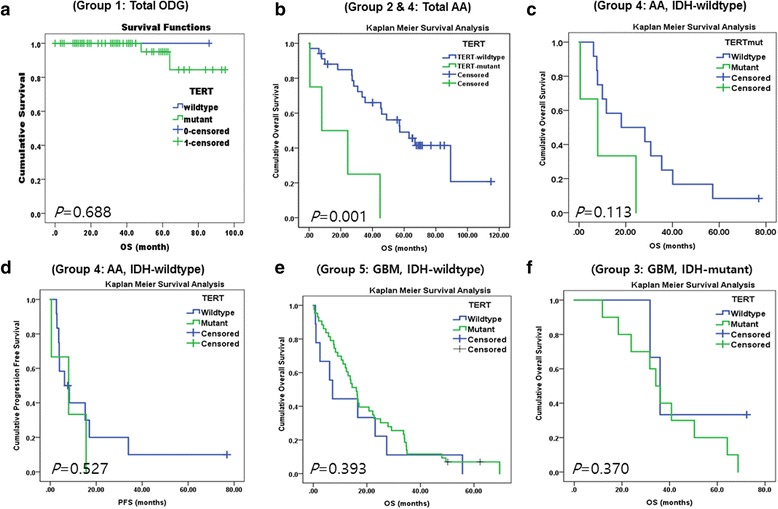
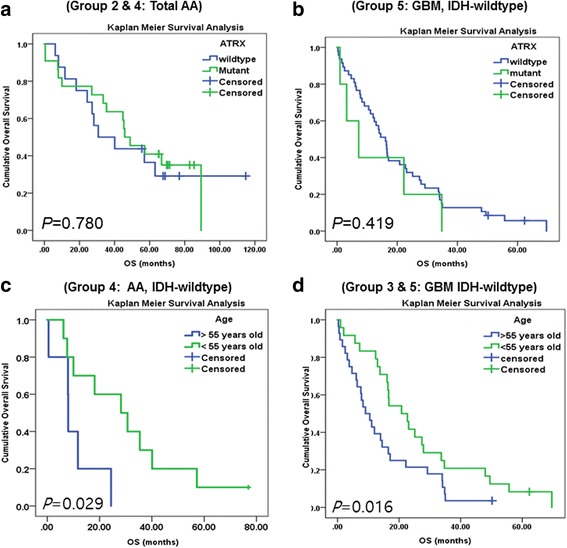
Mutations in the telomerase reverse transcriptase gene promoter (TERTp) are common in glioblastomas (GBMs) and oligodendrogliomas (ODGs), and therefore, have a key role in tumorigenesis and may be of prognostic value. However, the extent of their prognostic importance in various gliomas is controversial. We studied 168 patients separated into five groups: Group 1: 65 patients with ODG carrying an IDH1 or IDH2 mutation (IDH-mutant) and 1p/19q-codeletion, Group 2: 23 patients with anaplastic astrocytoma (AA), IDH-mutant, Group 3: 13 patients with GBM, IDH-mutant, Group 4: 15 patients with AA, IDH-wildtype (WT), and Group 5: 52 patients with GBM, IDH-WT. TERTp mutations were found in 96.9%, 4.4%, 76.9%, 20.0%, and 84.6% of patients in Groups 1, 2, 3, 4, and 5, respectively. The R132H mutation in IDH1 was found in 60.5% (23/38) of patients in the AA cohort (Groups 2 and 4) and 20.0% (13/65) of patients from our GBM cohort (Groups 3 and 5), whereas all patients with ODG (Group 1) had a mutation either in IDH1 (n = 62) or IDH2 (n = 3). Using Kaplan Meier survival analysis, we found that the TERTp mutation was correlated with poor overall survival (OS) in Groups 2 and 4 combined (P = 0.001) and in Group 4 (P = 0.113), and in multivariate analysis, the TERTp mutant group was associated with significantly poor survival in Group 5 (P = 0.045). However, IDH mutation, MGMT methylation, and younger patient age (<55 years old) were significantly correlated with favorable OS (all P < 0.05) in our cohort of astrocytic and ODGs. In patients with ODG (Group 1), mutant IDH and TERTp did not have prognostic value because these mutations were universally present. Based on the revised 2016 WHO classification of gliomas, we found that TERTp mutation was frequently present in patients with GBM or ODG and because it was strongly correlated with poor survival outcome in patients with IDH-WT GBM in multivariate analysis, it may be of prognostic value in this subgroup of patients with gliomas.
Keywords: Alpha-thalassemia/mental retardation syndrome X-linked (ATRX); Anaplastic astrocytoma; Glioblastoma; Isocitrate dehydrogenase (IDH); Oligodendroglioma; Telomerase reverse transcriptase.
Conflict of interest statement
Ethics approval and consent to participate
This study followed the principles of the World Medical Association Declaration of Helsinki and it was approved by the Institutional Review Board of SNUH (IRB No.: 1307-093-505).
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Clinical implications of TERT promoter mutation on IDH mutation and MGMT promoter methylation in diffuse gliomas.Pathol Res Pract. 2018 Jun;214(6):881-888. doi: 10.1016/j.prp.2018.04.002. Epub 2018 Apr 5. Pathol Res Pract. 2018. PMID: 29650441
-
Clinical insights gained by refining the 2016 WHO classification of diffuse gliomas with: EGFR amplification, TERT mutations, PTEN deletion and MGMT methylation.BMC Cancer. 2019 Oct 17;19(1):968. doi: 10.1186/s12885-019-6177-0. BMC Cancer. 2019. PMID: 31623593 Free PMC article.
-
Use of telomerase promoter mutations to mark specific molecular subsets with reciprocal clinical behavior in IDH mutant and IDH wild-type diffuse gliomas.J Neurosurg. 2018 Apr;128(4):1102-1114. doi: 10.3171/2016.11.JNS16973. Epub 2017 Jun 16. J Neurosurg. 2018. PMID: 28621624
-
IDH-mutant diffuse gliomas: tips and tricks in the era of genomic tumor classification.Histol Histopathol. 2023 Jul;38(7):739-753. doi: 10.14670/HH-18-582. Epub 2023 Jan 9. Histol Histopathol. 2023. PMID: 36651583 Review.
-
Correlation between IDH, ATRX, and TERT promoter mutations in glioma.Brain Tumor Pathol. 2020 Apr;37(2):33-40. doi: 10.1007/s10014-020-00360-4. Epub 2020 Mar 29. Brain Tumor Pathol. 2020. PMID: 32227259 Review.
Cited by
-
Drosophila melanogaster as a Model System for Human Glioblastomas.Adv Exp Med Biol. 2019;1167:207-224. doi: 10.1007/978-3-030-23629-8_12. Adv Exp Med Biol. 2019. PMID: 31520357 Review.
-
An expanded role for surgery in grade 3 1p/19q co-deleted oligodendroglioma.Neurooncol Adv. 2023 Apr 21;5(1):vdad046. doi: 10.1093/noajnl/vdad046. eCollection 2023 Jan-Dec. Neurooncol Adv. 2023. PMID: 37215951 Free PMC article.
-
TERTp Mutation and its Prognostic Value in Glioma Patients Under the 2021 WHO Classification: A Real-World Study.Cancer Med. 2025 Jan;14(2):e70533. doi: 10.1002/cam4.70533. Cancer Med. 2025. PMID: 39804195 Free PMC article.
-
Beyond IDH-Mutation: Emerging Molecular Diagnostic and Prognostic Features in Adult Diffuse Gliomas.Cancers (Basel). 2020 Jul 6;12(7):1817. doi: 10.3390/cancers12071817. Cancers (Basel). 2020. PMID: 32640746 Free PMC article. Review.
-
TERT Promoter Mutation in Benign and Malignant Salivary Gland Tumors; A Cross-Sectional Study.Iran J Pathol. 2023;18(1):64-74. doi: 10.30699/IJP.ijp.2023.556651.2927. Epub 2023 Mar 23. Iran J Pathol. 2023. PMID: 37383158 Free PMC article.
References
-
- Andersson U, Osterman P, Sjostrom S, Johansen C, Henriksson R, Brannstrom T, Broholm H, Christensen HC, Ahlbom A, Auvinen A, et al. MNS16A minisatellite genotypes in relation to risk of glioma and meningioma and to glioblastoma outcome. Int J Cancer. 2009;125:968–972. doi: 10.1002/ijc.24363. - DOI - PubMed
-
- Arita H, Narita Y, Fukushima S, Tateishi K, Matsushita Y, Yoshida A, Miyakita Y, Ohno M, Collins VP, Kawahara N, et al. Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 2013;126:267–276. doi: 10.1007/s00401-013-1141-6. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
