

Open vascular treatment of median arcuate ligament syndrome
- PMID: 28851450
- PMCID: PMC5575896
- DOI: 10.1186/s12893-017-0289-8
Open vascular treatment of median arcuate ligament syndrome
Abstract
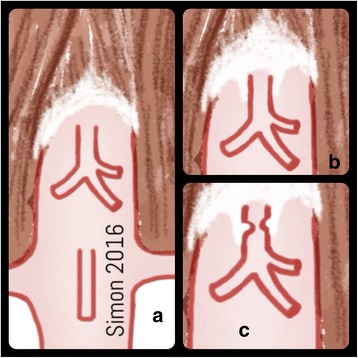
Background: Median arcuate ligament syndrome is a rare condition with abdominal symptoms. Accepted treatment options are open release of median arcuate ligament, laparoscopic release of edian arcuate ligament, robot-assisted release of median arcuate ligament and open vascular treatment. Here we aimed to evaluate the central priority of open vascular therapy in the treatment of median arcuate ligament syndrome.
Methods: We conducted a monocentric retrospective study between January 1996 and June 2016. Thirty-one patients with median arcuate ligament syndrome underwent open vascular surgery, including division of median arcuate ligament in 17 cases, and vascular reconstruction of the celiac artery in 14 cases.
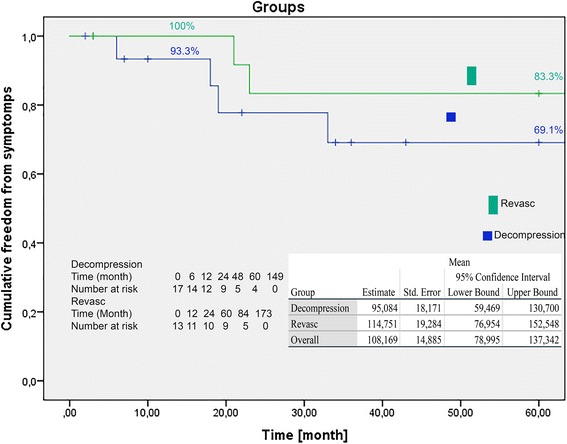
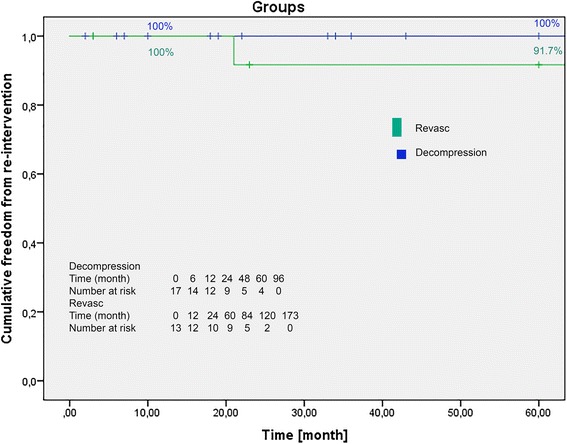
Results: In a 20-year period, 31 patients (n = 26 women, n = 5 men) were treated with division of median arcuate ligament (n = 17) or vascular reconstruction in combination with division of median arcuate ligament (n = 14). The mean age of patients was 44.8 ± 15.13 years. The complication rate was 16.1% (n = 5). Revisions were performed in 4 cases. The 30-day mortality rate was 0%. The mean in-hospital stay was 10.7 days. Follow-up data were obtained for 30 patients. The mean follow-up period was 52.2 months (range 2-149 months). Patients were grouped into a decompression group (n = 17) and revascularisation group (n = 13). The estimated Freedom From Symptoms rates were 93.3, 77.8, and 69.1% for the decompression group and 100, 83.3, and 83.3% for the revascularisation group after 12, 24 and 60 months respectively. We found no significant difference in the Freedom From Re-Intervention CA rates of the decompression (100% at 12, 24 and 60 months post-surgery) and revascularisation (100% at 12 months, and 91.7% at 24 and 60 months post-surgery) groups during follow-up (p = 0.26).
Conclusions: Open vascular treatment of median arcuate ligament syndrome is a safe, low mortality-risk procedure, with low morbidity rate. Treatment choice depends on the clinical and morphological situation of each patient.
Keywords: Celiac artery; Celiac artery compression syndrome; Dunbar syndrome; Intestinal ischemia; Median arcuate ligament syndrome.
Conflict of interest statement
Ethics approval and consent to participate
Retrospective data analysis was approved by the review board of the University of Düsseldorf (study number 5617). Patient informed consent was waived because of the retrospective characteristics of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Plate G, Eklöf B, Vang J. The celiac compression syndrome: myth or reality? Acta Chir Scand. 1981;147:201–203. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
