

The Second-Generation PGI2 Analogue Treprostinil Fails to Chemoprevent Tumors in a Murine Lung Adenocarcinoma Model
- PMID: 28851689
- PMCID: PMC5769875
- DOI: 10.1158/1940-6207.CAPR-17-0050
The Second-Generation PGI2 Analogue Treprostinil Fails to Chemoprevent Tumors in a Murine Lung Adenocarcinoma Model
Abstract
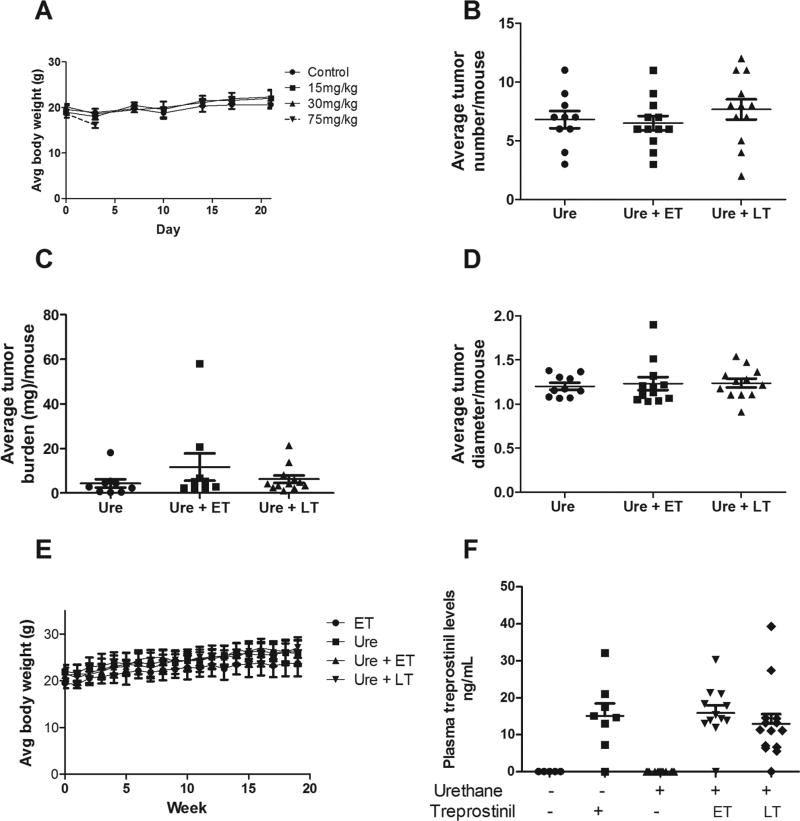
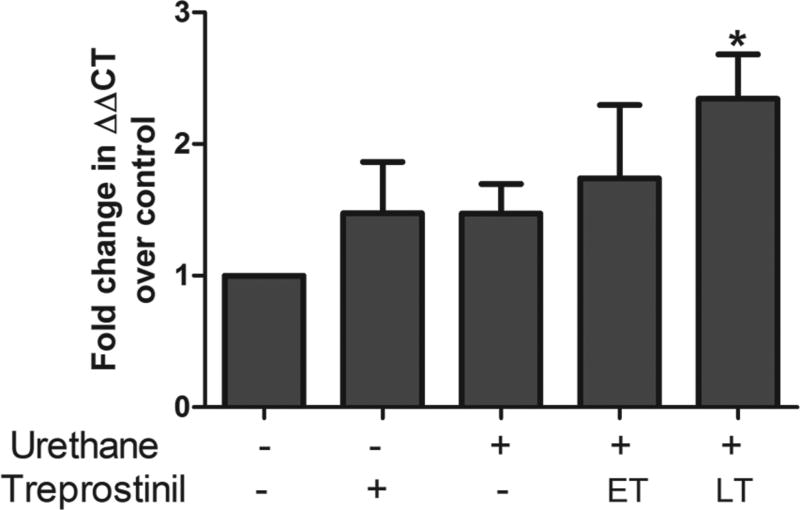
Prostacyclin (prostaglandin I2, PGI2) overproduction in FVB/N mice prevents the formation of carcinogen and tobacco smoke-induced adenomas, and administration of the oral prostacyclin analogue iloprost to wild-type mice also prevented carcinogen-induced mouse lung adenoma formation. Former smokers taking oral iloprost showed improved bronchial dysplasia histology compared with placebo. Next-generation oral prostacyclin analogues, like treprostinil, were developed for the treatment of pulmonary arterial hypertension (PAH). On the basis of our prior studies with iloprost, we performed preclinical studies examining the ability of treprostinil to chemoprevent urethane-induced murine lung adenocarcinoma. We determined the MTD in chow (prior studies had delivered treprostinil by gavage), and this dose produced serum levels in the experimental animals similar to those found in PAH patients treated with treprostinil. We then examined the chemopreventive efficacy of treprostinil exposure initiated both before (1 week) and after (6 weeks) urethane exposure to better model chemoprevention studies conducted in former smokers. Neither of these dosing strategies prevented murine lung cancer; however, we did detect changes in pulmonary inflammatory cell infiltrate and expression of CXCR4 (a chemokine receptor previously shown to increase in response to treprostinil exposure) in tumor-bearing, treprostinil-treated animals, indicating that the drug was bioavailable. One potential explanation stems from iloprost and treprostinil differentially activating cell surface prostaglandin receptors and intracellular peroxisome proliferator-activated receptors. When murine lung tumor cells were treated with treprostinil, their proliferation rate increased; in contrast, iloprost had no effect on proliferation. Future investigations comparing these two agents will provide insight into iloprost's chemopreventive mechanisms. Cancer Prev Res; 10(11); 671-9. ©2017 AACR.
©2017 American Association for Cancer Research.
Figures



Similar articles
-
Prostacyclin and EMT Pathway Markers for Monitoring Response to Lung Cancer Chemoprevention.Cancer Prev Res (Phila). 2018 Oct;11(10):643-654. doi: 10.1158/1940-6207.CAPR-18-0052. Epub 2018 Jul 25. Cancer Prev Res (Phila). 2018. PMID: 30045935 Free PMC article.
-
A comparative study of PGI2 mimetics used clinically on the vasorelaxation of human pulmonary arteries and veins, role of the DP-receptor.Prostaglandins Other Lipid Mediat. 2013 Dec;107:48-55. doi: 10.1016/j.prostaglandins.2013.07.001. Epub 2013 Jul 12. Prostaglandins Other Lipid Mediat. 2013. PMID: 23850788
-
Prostacyclin prevents murine lung cancer independent of the membrane receptor by activation of peroxisomal proliferator--activated receptor gamma.Cancer Prev Res (Phila). 2008 Oct;1(5):349-56. doi: 10.1158/1940-6207.CAPR-08-0145. Cancer Prev Res (Phila). 2008. PMID: 19138979 Free PMC article.
-
Cost effectiveness of prostacyclins in pulmonary arterial hypertension.Appl Health Econ Health Policy. 2012 May 1;10(3):175-88. doi: 10.2165/11630780-000000000-00000. Appl Health Econ Health Policy. 2012. PMID: 22452448 Review.
-
The potential for inhaled treprostinil in the treatment of pulmonary arterial hypertension.Ther Adv Respir Dis. 2011 Jun;5(3):195-206. doi: 10.1177/1753465810397693. Epub 2011 Feb 7. Ther Adv Respir Dis. 2011. PMID: 21300738 Review.
Cited by
-
Iloprost requires the Frizzled-9 receptor to prevent lung cancer.iScience. 2022 May 23;25(6):104442. doi: 10.1016/j.isci.2022.104442. eCollection 2022 Jun 17. iScience. 2022. PMID: 35707728 Free PMC article.
-
A Mixture of Baicalein, Wogonin, and Oroxylin-A Inhibits EMT in the A549 Cell Line via the PI3K/AKT-TWIST1-Glycolysis Pathway.Front Pharmacol. 2022 Feb 9;12:821485. doi: 10.3389/fphar.2021.821485. eCollection 2021. Front Pharmacol. 2022. PMID: 35222014 Free PMC article.
-
International Union of Basic and Clinical Pharmacology. CIX. Differences and Similarities between Human and Rodent Prostaglandin E2 Receptors (EP1-4) and Prostacyclin Receptor (IP): Specific Roles in Pathophysiologic Conditions.Pharmacol Rev. 2020 Oct;72(4):910-968. doi: 10.1124/pr.120.019331. Pharmacol Rev. 2020. PMID: 32962984 Free PMC article.
-
TARGETING THE PROSTACYCLIN/PEROXISOME PROLIFERATOR-ACTIVATED RECEPTOR GAMMA AXIS IN LUNG CANCER CHEMOPREVENTION.Trans Am Clin Climatol Assoc. 2018;129:48-55. Trans Am Clin Climatol Assoc. 2018. PMID: 30166698 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Lippman SM, Lee JJ, Karp DD, Vokes EE, Benner SE, Goodman GE, et al. Randomized phase III intergroup trial of isotretinoin to prevent second primary tumors in stage I non-small-cell lung cancer. J Natl Cancer Inst. 2001;93:605–18. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
