

Rare genetic variants in Shiga toxin-associated haemolytic uraemic syndrome: genetic analysis prior to transplantation is essential
- PMID: 28852487
- PMCID: PMC5569917
- DOI: 10.1093/ckj/sfx030
Rare genetic variants in Shiga toxin-associated haemolytic uraemic syndrome: genetic analysis prior to transplantation is essential
Abstract
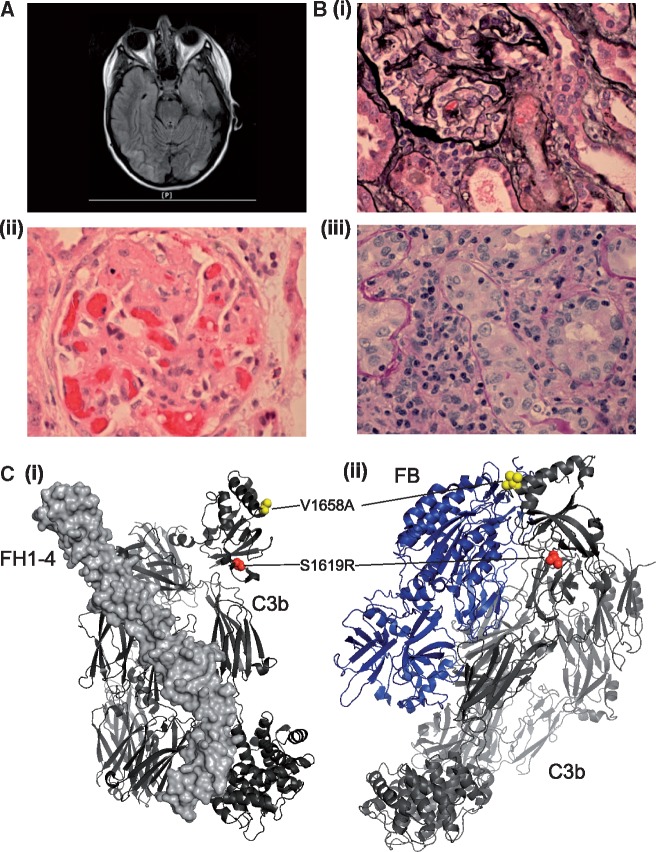
We present a case of haemolytic uraemic syndrome (HUS) in a 16-year-old female with serological evidence of acute Escherichia coli O157:H7 infection. She progressed to established renal failure and received a deceased donor kidney transplant. Shiga toxin-associated HUS (STEC-HUS) does not recur following renal transplantation, but unexpectedly this patient did experience rapid and severe HUS recurrence. She responded to treatment with the terminal complement inhibitor eculizumab and subsequent genetic analysis revealed a rare variant in a complement gene. This highlights the importance of genetic analysis in patients with STEC-HUS prior to renal transplantation so that management can be individualized.
Keywords: STEC-HUS; atypical haemolytic uraemic syndrome; complement; eculizumab; renal transplantation.
Figures
References
-
- Tarr PI, Gordon CA, Chandler WL.. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet 2005, 365: 1073–1086 - PubMed
-
- Siegler R, Oakes R.. Hemolytic uremic syndrome; pathogenesis, treatment, and outcome. Curr Opin Pediatr 2005; 17: 200–204 - PubMed
-
- Sheerin NS, Kavanagh D, Goodship TH. et al. A national specialized service in England for atypical haemolytic uraemic syndrome–the first year's experience. QJM 2016; 109: 27–33 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
