

Bundle in the Bronx: Impact of a Transition-of-Care Outpatient Parenteral Antibiotic Therapy Bundle on All-Cause 30-Day Hospital Readmissions
- PMID: 28852672
- PMCID: PMC5570156
- DOI: 10.1093/ofid/ofx097
Bundle in the Bronx: Impact of a Transition-of-Care Outpatient Parenteral Antibiotic Therapy Bundle on All-Cause 30-Day Hospital Readmissions
Abstract
Background: A streamlined transition from inpatient to outpatient care can decrease 30-day readmissions. Outpatient parenteral antibiotic therapy (OPAT) programs have not reduced readmissions; an OPAT bundle has been suggested to improve outcomes. We implemented a transition-of-care (TOC) OPAT bundle and assessed the effects on all-cause, 30-day hospital readmission.
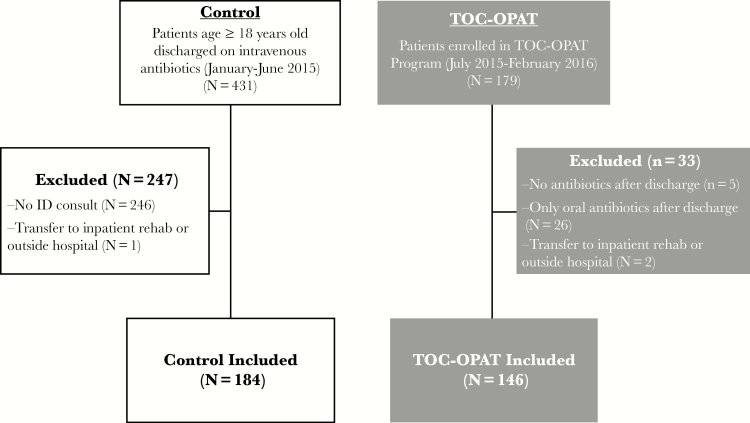
Methods: Retrospectively, patients receiving postdischarge intravenous antibiotics were evaluated before and after implementation of a TOC-OPAT program in Bronx, New York, between July, 2015 and February, 2016. Pearson's χ2 test was used to compare 30-day readmissions between groups, and logistic regression was used to adjust for covariates. Time from discharge to readmission was analyzed to assess readmission risk, using log-rank test to compare survival curves and Cox proportional hazards model to adjust for covariates. Secondary outcomes, 30-day emergency department (ED) visits, and mortality were analyzed similarly.
Results: Compared with previous standard care (n = 184), the TOC-OPAT group (n = 146) had significantly lower 30-day readmissions before (13.0% vs 26.1%, P < .01) and after adjustment for covariates (odds ratio [OR] = 0.51; 95% confidence interval [CI], 0.27-0.94; P = .03). In time-dependent analyses, TOC-OPAT patients were at significantly lower risk for readmission (log-rank test, P < .01; hazard ratio = 0.56; 95% CI, 0.32-0.97; P = .04). Propensity-matched sensitivity analysis showed lower readmissions in the TOC-OPAT group (13.6% vs 24.6%, P = .04), which was attenuated after adjustment (OR = 0.51; 95% CI, 0.25-1.05; P = .07). Mortality and ED visits were similar in both groups.
Conclusions: Our TOC-OPAT patients had reduced 30-day readmissions compared with the previous standard of care. An effective TOC-OPAT bundle can successfully improve patient outcomes in an economically disadvantaged area.
Keywords: bundle; outpatient parenteral antibiotic therapy; readmission; transitional care model..
Figures
References
-
- Balinsky W, Nesbitt S. Cost-effectiveness of outpatient parenteral antibiotics: a review of the literature. Am J Med 1989; 87:301–5. - PubMed
-
- Grayson ML, Silvers J, Turnidge J. Home intravenous antibiotic therapy. A safe and effective alternative to inpatient care. Med J Aust 1995; 162:249–53. - PubMed
-
- Dalovisio JR, Juneau J, Baumgarten K, Kateiva J. Financial impact of a home intravenous antibiotic program on a medicare managed care program. Clin Infect Dis 2000; 30:639–42. - PubMed
-
- Ruh CA, Parameswaran GI, Wojciechowski AL, Mergenhagen KA. Outcomes and pharmacoeconomic analysis of a home intravenous antibiotic infusion program in veterans. Clin Ther 2015; 37:2527–35. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
