

Thyroid diseases and bone health
- PMID: 28853052
- PMCID: PMC5754375
- DOI: 10.1007/s40618-017-0753-4
Thyroid diseases and bone health
Abstract
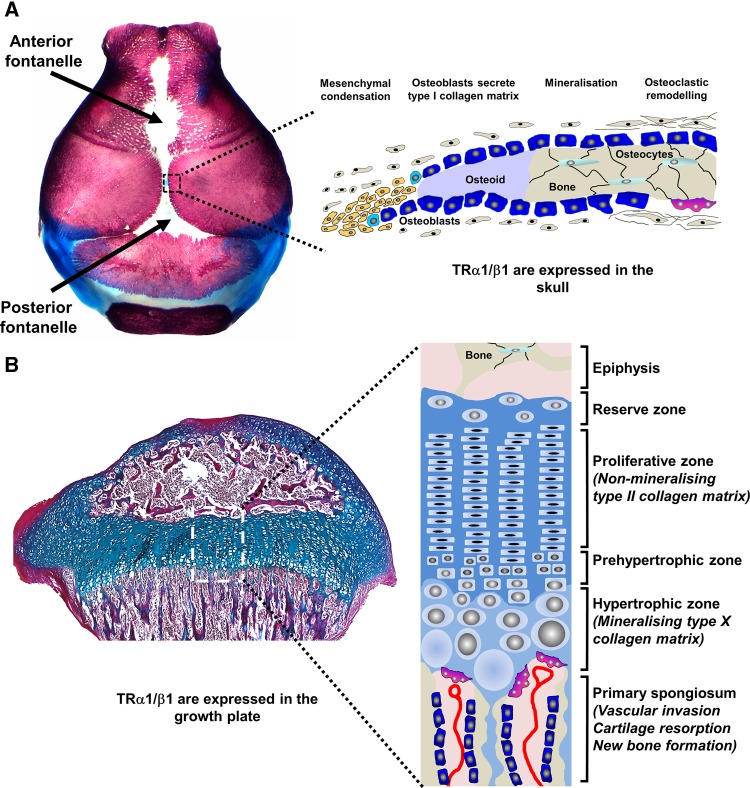
Thyroid hormones are essential for skeletal development and are important regulators of bone maintenance in adults. Childhood hypothyroidism causes delayed skeletal development, retarded linear growth and impaired bone mineral accrual. Epiphyseal dysgenesis is evidenced by classic features of stippled epiphyses on X-ray. In severe cases, post-natal growth arrest results in a complex skeletal dysplasia. Thyroid hormone replacement stimulates catch-up growth and bone maturation, but recovery may be incomplete dependent on the duration and severity of hypothyroidism prior to treatment. A severe phenotype characteristic of hypothyroidism occurs in children with resistance to thyroid hormone due to mutations affecting THRA encoding thyroid hormone receptor α (TRα). Discovery of this rare condition recapitulated animal studies demonstrating that TRα mediates thyroid hormone action in the skeleton. In adults, thyrotoxicosis is well known to cause severe osteoporosis and fracture, but cases are rare because of prompt diagnosis and treatment. Recent data, however, indicate that subclinical hyperthyroidism is associated with low bone mineral density (BMD) and an increased risk of fracture. Population studies have also shown that variation in thyroid status within the reference range in post-menopausal women is associated with altered BMD and fracture risk. Thus, thyroid status at the upper end of the euthyroid reference range is associated with low BMD and increased risk of osteoporotic fragility fracture. Overall, extensive data demonstrate that euthyroid status is required for normal post-natal growth and bone mineral accrual, and is fundamental for maintenance of adult bone structure and strength.
Keywords: Bone development; Hypothyroidism; Osteoporosis; Thyroid hormone receptor α; Thyrotoxicosis.
Conflict of interest statement
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
No informed consent.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
