

HIV, violence, blame and shame: pathways of risk to internalized HIV stigma among South African adolescents living with HIV
- PMID: 28853517
- PMCID: PMC5577824
- DOI: 10.7448/IAS.20.1.21771
HIV, violence, blame and shame: pathways of risk to internalized HIV stigma among South African adolescents living with HIV
Abstract
Introduction: Internalized HIV stigma is a key risk factor for negative outcomes amongst adolescents living with HIV (ALHIV), including non-adherence to anti-retroviral treatment, loss-to-follow-up and morbidity. This study tested a theoretical model of multi-level risk pathways to internalized HIV stigma among South African ALHIV.
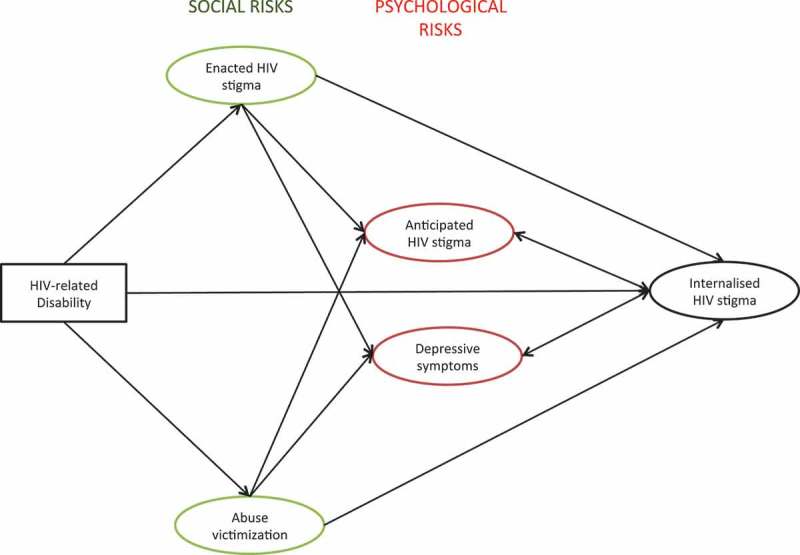
Methods: From 2013 to 2015, a survey using total population sampling of ALHIV who had ever initiated anti-retroviral treatment (ART) in 53 public health facilities in the Eastern Cape, South Africa was conducted. Community-tracing ensured inclusion of ALHIV who were defaulting from ART or lost to follow-up. 90.1% of eligible ALHIV were interviewed (n = 1060, 55% female, mean age = 13.8, 21% living in rural locations). HIV stigma mechanisms (internalized, enacted, and anticipated), HIV-related disability, violence victimization (physical, emotional, sexual abuse, bullying victimization) were assessed using well-validated self-report measures. Structural equation modelling was used to test a theoretically informed model of risk pathways from HIV-related disability to internalized HIV stigma. The model controlled for age, gender and urban/rural address.
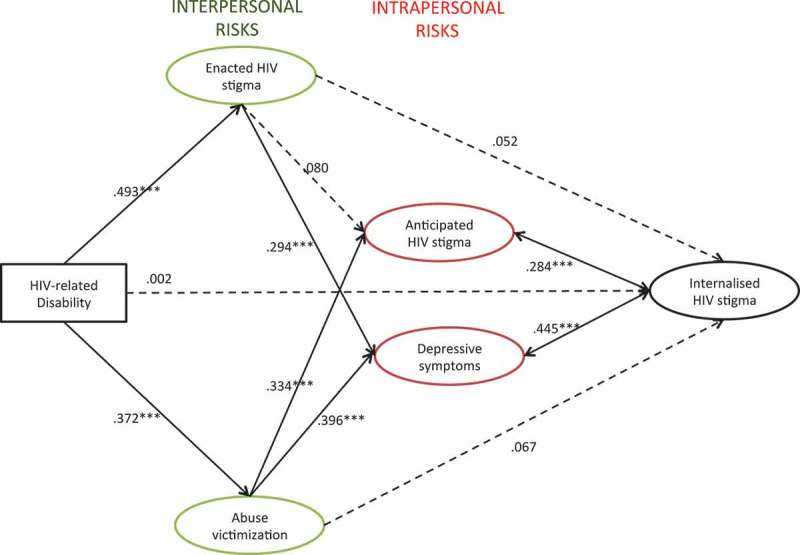
Results: Prevalence of internalized HIV stigma was 26.5%. As hypothesized, significant associations between internalized stigma and anticipated stigma, as well as depression were obtained. Unexpectedly, HIV-related disability, victimization, and enacted stigma were not directly associated with internalized stigma. Instead significant pathways were identified via anticipated HIV stigma and depression. The model fitted the data well (RMSEA = .023; CFI = .94; TLI = .95; WRMR = 1.070).
Conclusions: These findings highlight the complicated nature of internalized HIV stigma. Whilst it is seemingly a psychological process, indirect pathways suggest multi-level mechanisms leading to internalized HIV stigma. Findings suggest that protection from violence within homes, communities and schools may interrupt risk pathways from HIV-related health problems to psychological distress and internalized HIV stigma. This highlights the potential for interventions that do not explicitly target adolescents living with HIV but are sensitive to their needs.
Keywords: HIV/AIDS; abuse; adolescent; shame; stigma; structural equation modelling.
Conflict of interest statement
MP has no competing interests to declare. MB has no competing interests to declare. LC has no competing interests to declare. FM has no competing interests to declare.
Figures
References
-
- Idele P, Gillespie A, Porth T, Suzuki C, Mahy M, Kasedde S, et al. Epidemiology of HIV and AIDS among adolescents: current status, inequities, and data gaps. J Acquir Immune Defic Syndr [Internet]. United States: Idele, Priscilla. *United Nations Children’s Fund, New York, NY; and +Joint United Nations Programme on HIV/AIDS, Geneva, Switzerland;2014;66(Suppl 2):S144–9. Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medl&NEWS=N&AN=... - PubMed
-
- World Health Organisation (WHO) Health for the world’s adolescents. Geneva: WHO; 2014.
-
- The United Nations Children's Fund (UNICEF) For every child, end AIDS: seventh stocktaking report. New York: UNICEF; 2016.
-
- Pantelic M, Shenderovich Y, Cluver L, Boyes M.. Predictors of internalised HIV-related stigma: a systematic review of studies in sub-Saharan Africa. Health Psychol Rev [Internet]. 2015. Jan:9(4):469–90. [cited 2016 February8] Available from: http://www.ncbi.nlm.nih.gov/pubmed/25559431 - PubMed
-
- Gross R, Yip B, Lo V, Iii R, Wood E, Alexander CS, et al. A simple, dynamic measure of antiretroviral therapy adherence predicts failure to maintain HIV-1 suppression. J Infect Dis. 2006;6021:1108–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
