

Adherence to Rivaroxaban, Dabigatran, and Apixaban for Stroke Prevention for Newly Diagnosed and Treatment-Naive Atrial Fibrillation Patients: An Update Using 2013-2014 Data
- PMID: 28854077
- PMCID: PMC5747360
- DOI: 10.18553/jmcp.2017.23.9.958
Adherence to Rivaroxaban, Dabigatran, and Apixaban for Stroke Prevention for Newly Diagnosed and Treatment-Naive Atrial Fibrillation Patients: An Update Using 2013-2014 Data
Abstract
Background: Few studies have assessed adherence to non-vitamin K antagonist oral anticoagulants (NOACs), especially using contemporary data now that multiple NOACs are available.
Objective: To compare adherence and treatment patterns among NOACs for stroke prevention in patients with nonvalvular atrial fibrillation (NVAF).
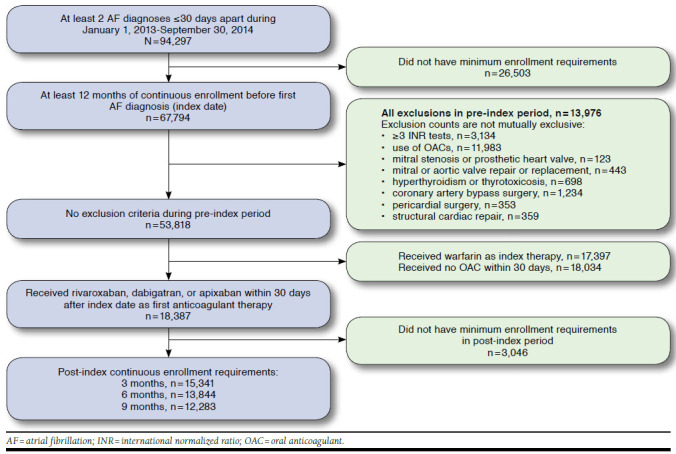
Methods: Incident and treatment-naive NVAF patients were identified during 2013-2014 from a large claims database in this retrospective cohort study. Patients were included who initiated rivaroxaban, dabigatran, or apixaban within 30 days after diagnosis. Adherence to the index medication and adherence to any oral anticoagulant was assessed using the proportion of days covered (PDC) at 3, 6, and 9 months. The number of switches and gaps in therapy were also evaluated. Analyses were stratified by stroke risk scores, and a logistic regression model was used to control for factors that may predict high adherence.
Results: Dabigatran had lower adherence (PDC = 0.76, 0.64, 0.57) compared with rivaroxaban (PDC = 0.83, 0.73, 0.66; P < 0.001) and apixaban (PDC = 0.82, 0.72, 0.66; P < 0.001) at 3, 6, and 9 months of follow-up and twice the number of switches to either other anticoagulants or antiplatelet therapy. Adherence was higher overall as stroke risk increased, and dabigatran had consistently lower adherence compared with the other NOACs. Multivariable logistic regression predicting PDC ≥ 0.80 showed rivaroxaban users with higher odds of high adherence compared with dabigatran or rivaroxaban across all time periods. Adjusted analyses showed that increasing age and comorbid hypertension and diabetes were associated with higher adherence.
Conclusions: In this real-world analysis of adherence to NOACs, rivaroxaban and apixaban had favorable unadjusted adherence profiles compared with dabigatran, while rivaroxaban users had higher odds of high adherence (PDC ≥ 0.80) among the NOACs in adjusted analyses. Clinicians and managed care organizations should consider the implications of lower adherence on clinical outcomes and quality assessment.
Disclosures: This project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant number UL1TR000117. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. The authors have nothing to disclose. Study concept and design were contributed by Brown and Shewale. Brown and Talbert collected the data, and data analysis was performed primarily by Brown, along with Shewale and Talbert. The manuscript was written primarily by Brown, along with Shewale, and revised by all the authors.
Conflict of interest statement
This project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant number UL1TR000117. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. The authors have nothing to disclose. Study concept and design were contributed by Brown and Shewale. Brown and Talbert collected the data, and data analysis was performed primarily by Brown, along with Shewale and Talbert. The manuscript was written primarily by Brown, along with Shewale, and revised by all the authors.
Similar articles
-
Adherence to Rivaroxaban, Dabigatran, and Apixaban for Stroke Prevention in Incident, Treatment-Naïve Nonvalvular Atrial Fibrillation.J Manag Care Spec Pharm. 2016 Nov;22(11):1319-1329. doi: 10.18553/jmcp.2016.22.11.1319. J Manag Care Spec Pharm. 2016. PMID: 27783556 Free PMC article.
-
Adherence to Rivaroxaban Compared with Other Oral Anticoagulant Agents Among Patients with Nonvalvular Atrial Fibrillation.J Manag Care Spec Pharm. 2017 Sep;23(9):980-988. doi: 10.18553/jmcp.2017.23.9.980. J Manag Care Spec Pharm. 2017. PMID: 28854075 Free PMC article.
-
Major Bleeding Risk During Anticoagulation with Warfarin, Dabigatran, Apixaban, or Rivaroxaban in Patients with Nonvalvular Atrial Fibrillation.J Manag Care Spec Pharm. 2017 Sep;23(9):968-978. doi: 10.18553/jmcp.2017.23.9.968. J Manag Care Spec Pharm. 2017. PMID: 28854073 Free PMC article.
-
Direct comparative effectiveness and safety between non-vitamin K antagonist oral anticoagulants for stroke prevention in nonvalvular atrial fibrillation: a systematic review and meta-analysis of observational studies.Eur J Epidemiol. 2019 Feb;34(2):173-190. doi: 10.1007/s10654-018-0415-7. Epub 2018 Jun 8. Eur J Epidemiol. 2019. PMID: 29948370
-
Cost-Effectiveness of Novel Oral Anticoagulants for Stroke Prevention in Non-Valvular Atrial Fibrillation.Curr Cardiol Rep. 2015 Aug;17(8):61. doi: 10.1007/s11886-015-0618-4. Curr Cardiol Rep. 2015. PMID: 26081245 Review.
Cited by
-
Reducing Stroke Risk in Atrial Fibrillation: Adherence to Guidelines Has Improved, but Patient Persistence with Anticoagulant Therapy Remains Suboptimal.Korean Circ J. 2019 Oct;49(10):883-907. doi: 10.4070/kcj.2019.0234. Korean Circ J. 2019. PMID: 31535493 Free PMC article. Review.
-
Role of the anticoagulant monitoring service in 2018: beyond warfarin.Hematology Am Soc Hematol Educ Program. 2018 Nov 30;2018(1):348-352. doi: 10.1182/asheducation-2018.1.348. Hematology Am Soc Hematol Educ Program. 2018. PMID: 30504331 Free PMC article. Review.
-
Adherence and persistence with direct oral anticoagulants by dose regimen: A systematic review.Br J Clin Pharmacol. 2025 Apr;91(4):1096-1113. doi: 10.1002/bcp.70003. Epub 2025 Feb 16. Br J Clin Pharmacol. 2025. PMID: 39957057 Free PMC article.
-
Estimating Adherence Based on Prescription or Dispensation Information: Impact on Thresholds and Outcomes. A Real-World Study With Atrial Fibrillation Patients Treated With Oral Anticoagulants in Spain.Front Pharmacol. 2018 Dec 3;9:1353. doi: 10.3389/fphar.2018.01353. eCollection 2018. Front Pharmacol. 2018. PMID: 30559661 Free PMC article.
-
Prevalence and Predictors of Nonadherence to Direct Oral Anticoagulant Treatment in Patients with Atrial Fibrillation.TH Open. 2023 Sep 27;7(3):e270-e279. doi: 10.1055/a-2161-0928. eCollection 2023 Jul. TH Open. 2023. PMID: 37772087 Free PMC article.
References
-
- Desai NR, Krumme AA, Schneeweiss S, et al. . Patterns of initiation of oral anticoagulants in patients with atrial fibrillation—quality and cost implications. Am J Med. 2014;127(11):1075-82.e1. - PubMed
-
- Ruff CT, Giugliano RP, Braunwald E, et al. . Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-62. - PubMed
-
- Adam SS, McDuffie JR, Ortel TL, Williams JW Jr. Comparative effectiveness of warfarin and new oral anticoagulants for the management of atrial fibrillation and venous thromboembolism: a systematic review. Ann Intern Med. 2012;157(11):796-807. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
