

Orthotopic patient-derived xenografts of paediatric solid tumours
- PMID: 28854174
- PMCID: PMC5659286
- DOI: 10.1038/nature23647
Orthotopic patient-derived xenografts of paediatric solid tumours
Abstract
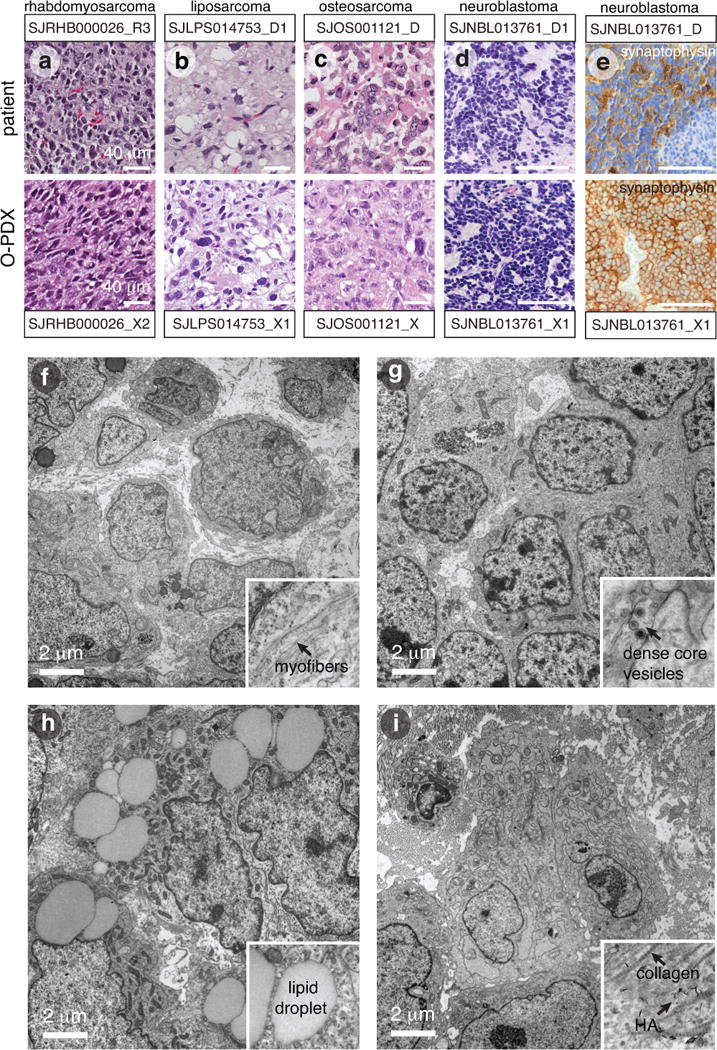
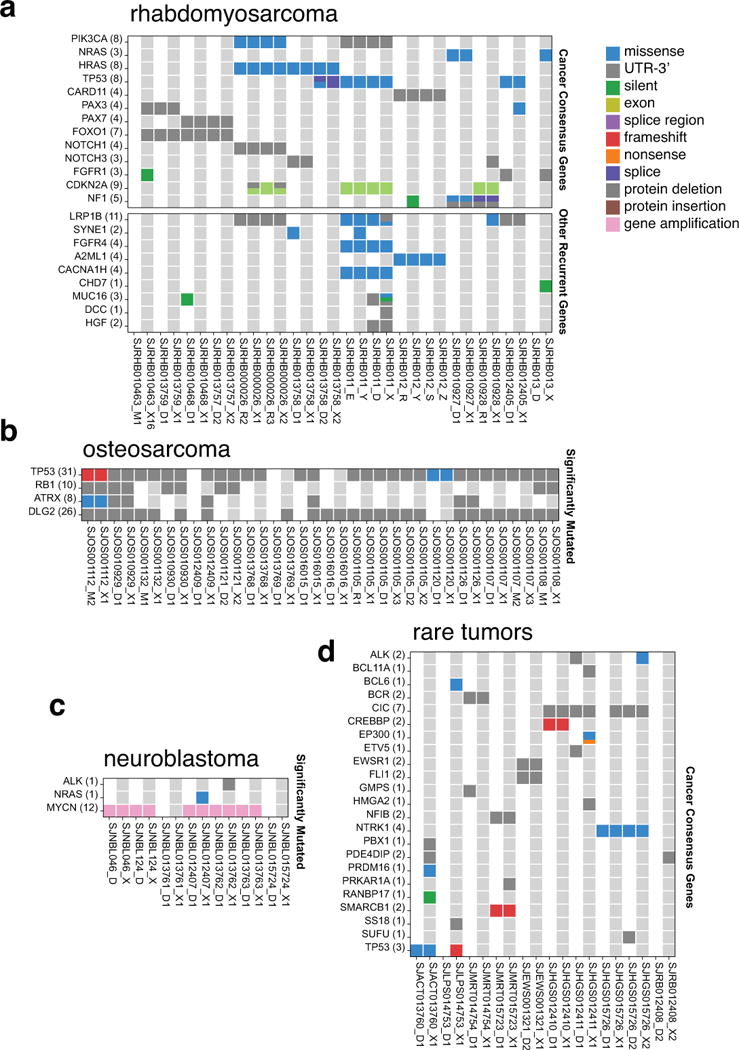
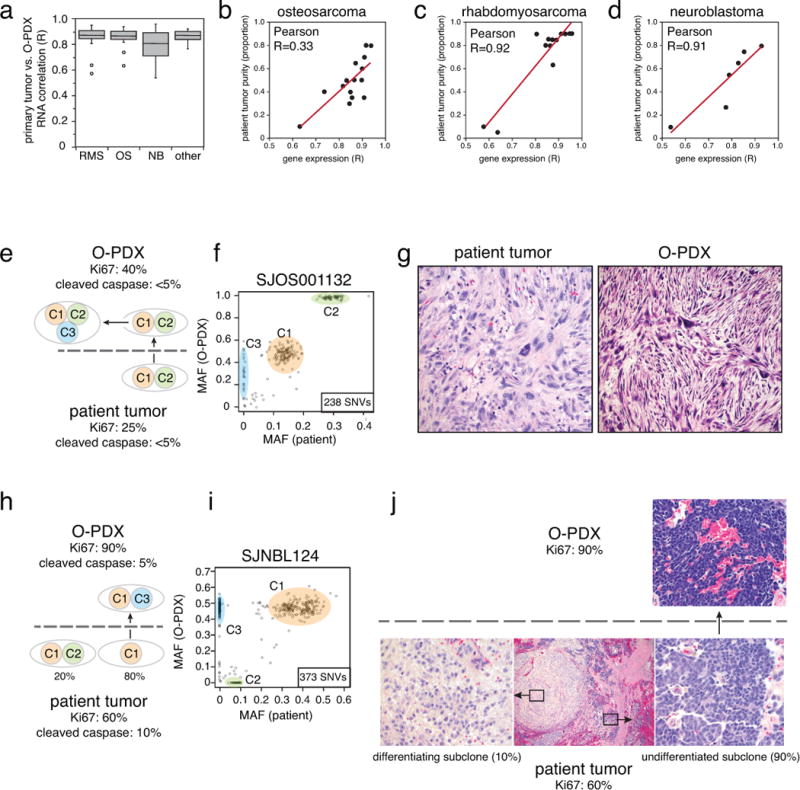
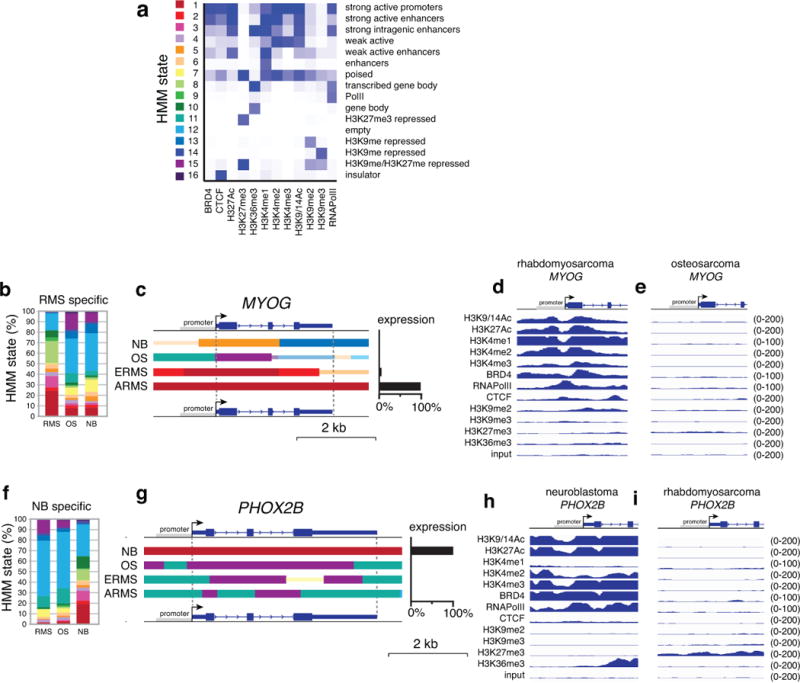
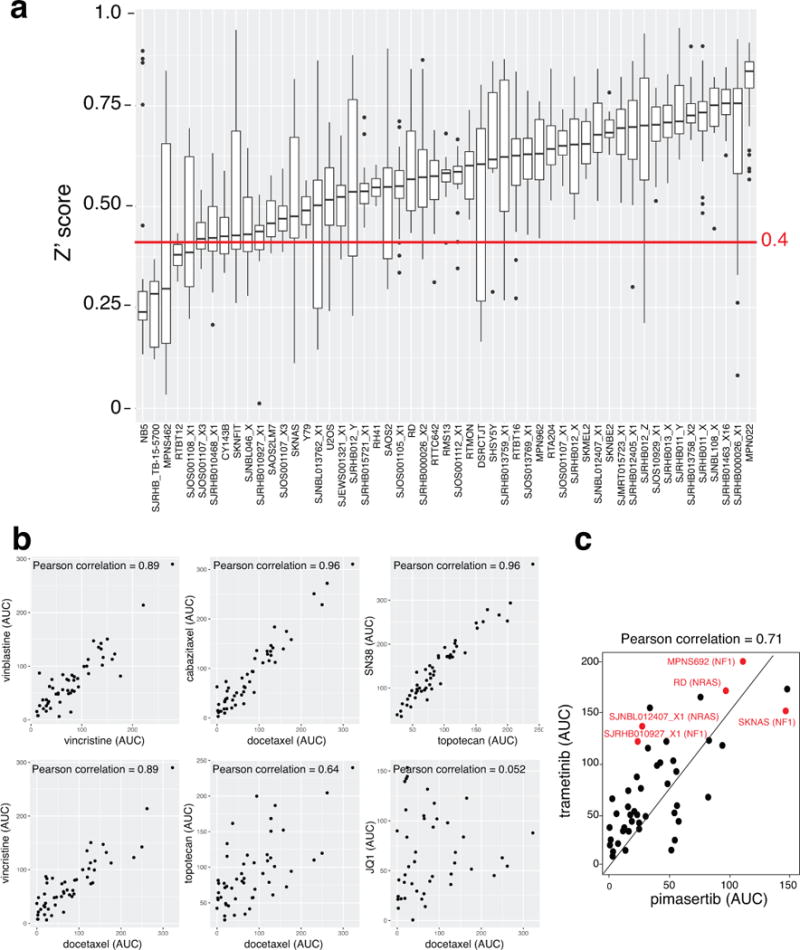
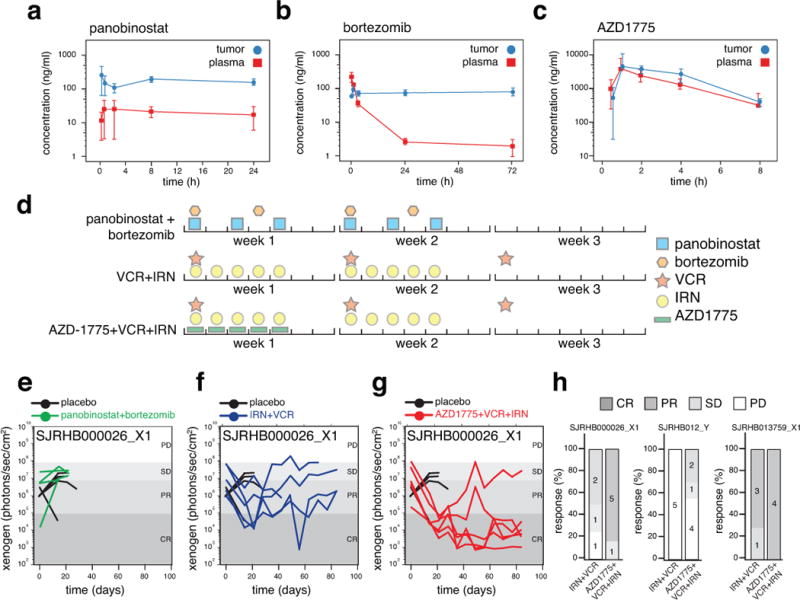
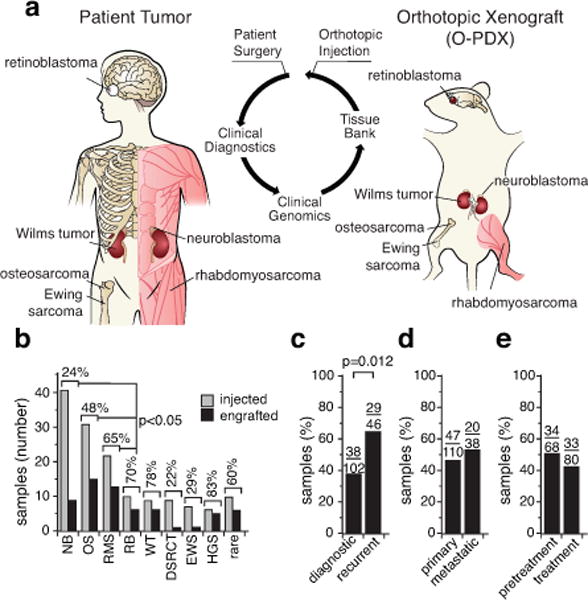
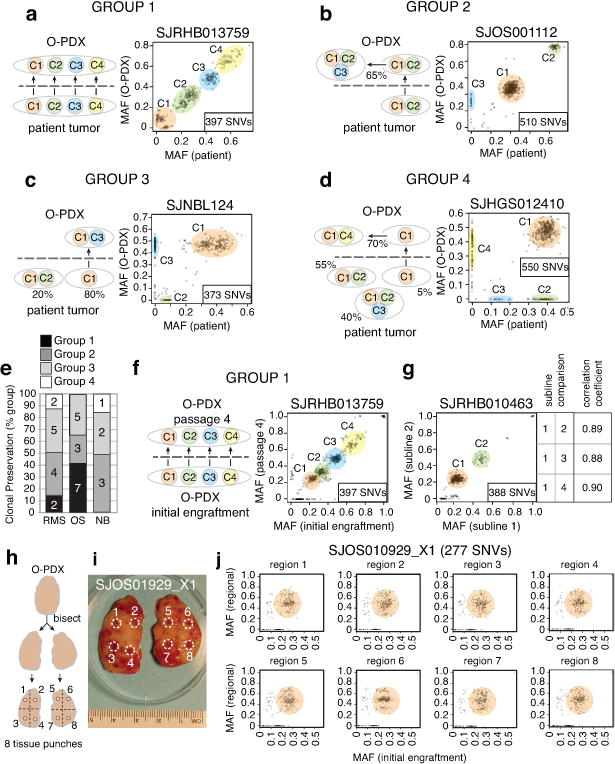
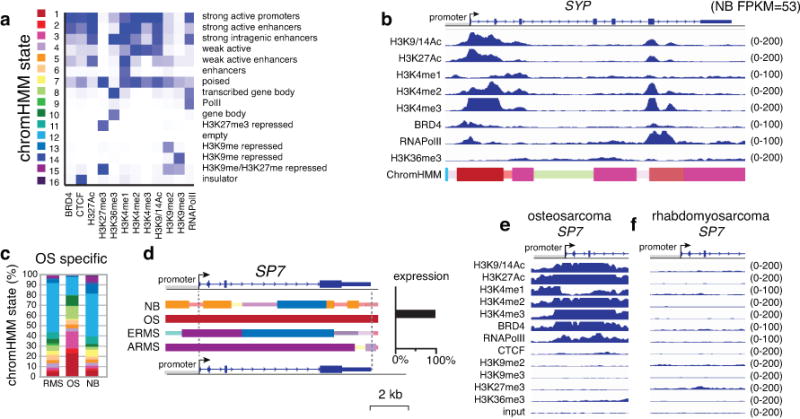
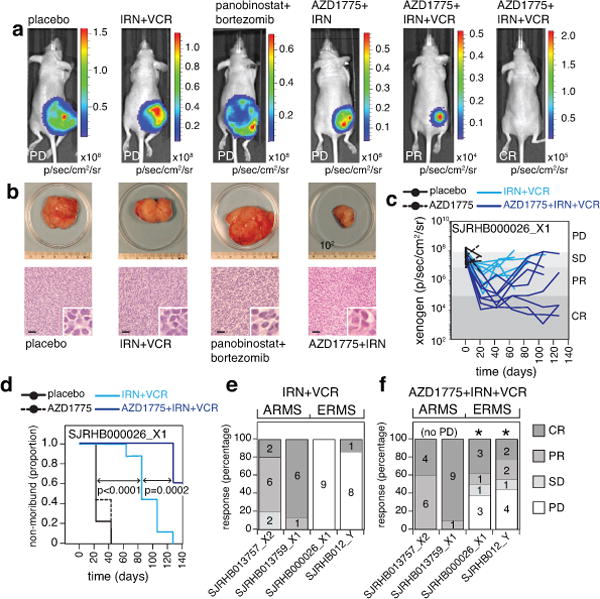
Paediatric solid tumours arise from endodermal, ectodermal, or mesodermal lineages. Although the overall survival of children with solid tumours is 75%, that of children with recurrent disease is below 30%. To capture the complexity and diversity of paediatric solid tumours and establish new models of recurrent disease, here we develop a protocol to produce orthotopic patient-derived xenografts at diagnosis, recurrence, and autopsy. Tumour specimens were received from 168 patients, and 67 orthotopic patient-derived xenografts were established for 12 types of cancer. The origins of the patient-derived xenograft tumours were reflected in their gene-expression profiles and epigenomes. Genomic profiling of the tumours, including detailed clonal analysis, was performed to determine whether the clonal population in the xenograft recapitulated the patient's tumour. We identified several drug vulnerabilities and showed that the combination of a WEE1 inhibitor (AZD1775), irinotecan, and vincristine can lead to complete response in multiple rhabdomyosarcoma orthotopic patient-derived xenografts tumours in vivo.
Conflict of interest statement
Figures
Comment in
-
Cancer models: The next best thing.Nature. 2017 Sep 7;549(7670):39-41. doi: 10.1038/nature23545. Epub 2017 Aug 30. Nature. 2017. PMID: 28854165 No abstract available.
