

Acute rhabdomyolysis and delayed pericardial effusion in an Italian patient with Ebola virus disease: a case report
- PMID: 28854896
- PMCID: PMC5576302
- DOI: 10.1186/s12879-017-2689-x
Acute rhabdomyolysis and delayed pericardial effusion in an Italian patient with Ebola virus disease: a case report
Abstract
Background: During the 2013-2016 West Africa Ebola virus disease (EVD) epidemic, some EVD patients, mostly health care workers, were evacuated to Europe and the USA.
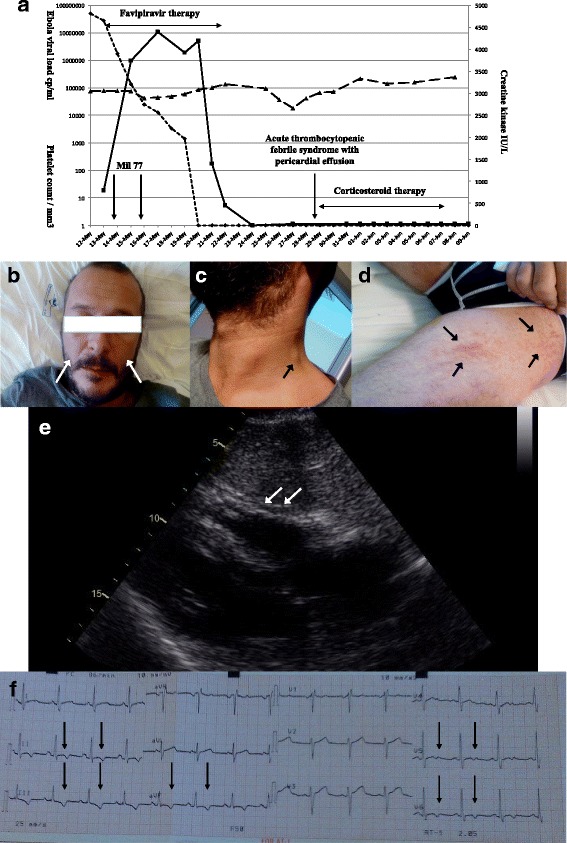
Case presentation: In May 2015, a 37-year old male nurse contracted Ebola virus disease in Sierra Leone. After Ebola virus detection in plasma, he was medically-evacuated to Italy. At admission, rhabdomyolysis was clinically and laboratory-diagnosed and was treated with aggressive hydration, oral favipiravir and intravenous investigational monoclonal antibodies against Ebola virus. The recovery clinical phase was complicated by a febrile thrombocytopenic syndrome with pericardial effusion treated with corticosteroids for 10 days and indomethacin for 2 months. No evidence of recurrence is reported.
Conclusions: A febrile thrombocytopenic syndrome with pericardial effusion during the recovery phase of EVD appears to be uncommon. Clinical improvement with corticosteroid treatment suggests that an immune-mediated mechanism contributed to the pericardial effusion.
Keywords: Ebola Virus Disease; Pericardial effusion; Rhabdomyolysis.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
The INMI’s Institutional Ethical Board assessed the criteria for access to experimental drugs and invasive procedures, approved informed consent form and analyzed ethical issues and possible solutions to minimize the physical and psychological harm for the patient. The patient signed an informed consent for any single procedure or treatment performed, after thoroughly explanation of reasonably anticipated benefits and potential hazards of intervention.
Emergency Use Authorization for investigational new drugs was issued by the Italian Drug Agency (AIFA), the authority entitled to approve medical agents to be used for therapy of disease when they are not the standard of care or supported by research that proves their safety.
Competing interests
The authors declare that they have no competing interest.
Disclaimer: The views expressed are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Cellarier GR, Bordes J, Karkowski L, Gagnon N, Billhot M, Cournac JM, et al. Safety, feasibility, and interest of transthoracic echocardiography in a deployed French military Ebola virus disease treatment center in Guinea. Intensive Care Med. 2015;41:1491–1492. doi: 10.1007/s00134-015-3821-2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
