

Reduced growth velocity across the third trimester is associated with placental insufficiency in fetuses born at a normal birthweight: a prospective cohort study
- PMID: 28854913
- PMCID: PMC5577811
- DOI: 10.1186/s12916-017-0928-z
Reduced growth velocity across the third trimester is associated with placental insufficiency in fetuses born at a normal birthweight: a prospective cohort study
Abstract
Background: While being small-for-gestational-age due to placental insufficiency is a major risk factor for stillbirth, 50% of stillbirths occur in appropriate-for-gestational-age (AGA, > 10th centile) fetuses. AGA fetuses are plausibly also at risk of stillbirth if placental insufficiency is present. Such fetuses may be expected to demonstrate declining growth trajectory across pregnancy, although they do not fall below the 10th centile before birth. We investigated whether reduced growth velocity in AGA fetuses is associated with antenatal, intrapartum and neonatal indicators of placental insufficiency.
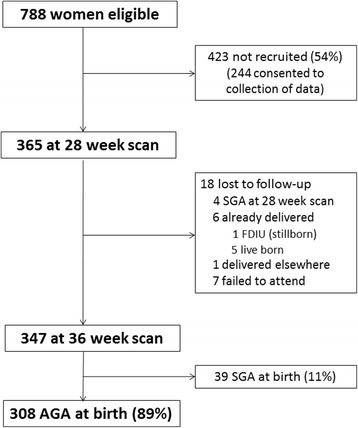
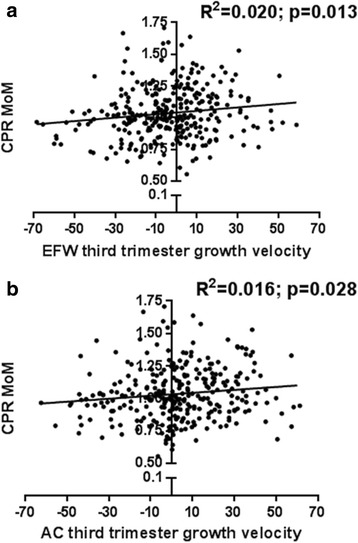
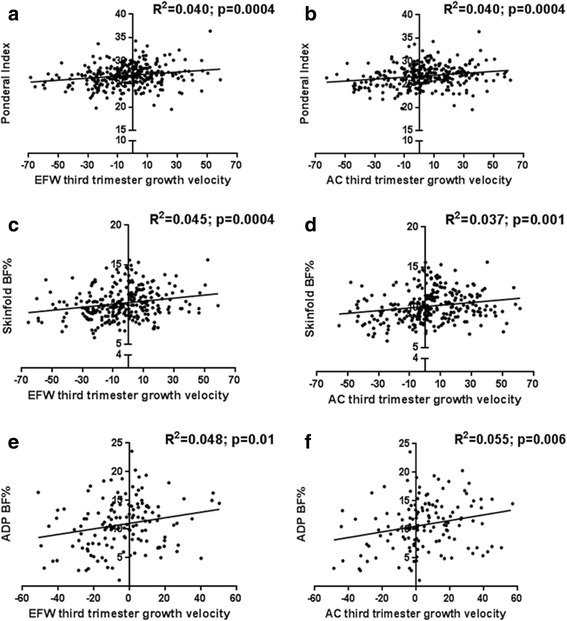
Methods: We performed a prospective cohort study of 308 nulliparous women who subsequently gave birth to AGA infants. Ultrasound was utilised at 28 and 36 weeks' gestation to determine estimated fetal weight (EFW) and abdominal circumference (AC). We correlated relative EFW and AC growth velocities with three clinical indicators of placental insufficiency, namely (1) fetal cerebroplacental ratio (CPR; CPR < 5th centile reflects placental resistance, and blood flow redistribution to the brain - a fetal response to hypoxia); (2) neonatal acidosis after the hypoxic challenge of labour (umbilical artery (UA) pH < 7.15 at birth); and (3) low neonatal body fat percentage (BF%, measured by air displacement plethysmography) reflecting reduced nutritional reserve in utero.
Results: For each one centile reduction in EFW growth velocity between 28 and 36 weeks' gestation, there was a 2.4% increase in the odds of cerebral redistribution (CPR < 5th centile, odds ratio (OR) (95% confidence interval) = 1.024 (1.005-1.042), P = 0.012) and neonatal acidosis (UA pH < 7.15, OR = 1.024 (1.003-1.046), P = 0.023), and a 3.3% increase in the odds of low BF% (OR = 1.033 (1.001-1.067), P = 0.047). A decline in EFW of > 30 centiles between 28 and 36 weeks (compared to greater relative growth) was associated with cerebral redistribution (CPR < 5th centile relative risk (RR) = 2.80 (1.25-6.25), P = 0.026), and a decline of > 35 centiles was associated with neonatal acidosis (UA pH < 7.15 RR = 3.51 (1.40-8.77), P = 0.030). Similar associations were identified between low AC growth velocity and clinical indicators of placental insufficiency.
Conclusions: Reduced growth velocity between 28 and 36 weeks' gestation among fetuses born AGA is associated with antenatal, intrapartum and neonatal indicators of placental insufficiency. These fetuses potentially represent an important unrecognised cohort at increased risk of stillbirth and may warrant more intensive antenatal surveillance.
Keywords: Appropriate-for-gestational-age; Birthweight; Cerebroplacental ratio; Fetal growth restriction; Growth trajectory; Growth velocity; Placental insufficiency; Prenatal; Small-for-gestational-age; Stillbirth; Ultrasonography.
Conflict of interest statement
Ethics approval and consent to participate
Written informed consent was obtained from all participants, and this study was approved by the Mercy Health Research Ethics Committee, Ethics Approval Number R14/12.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Reduced growth velocity from the mid-trimester is associated with placental insufficiency in fetuses born at a normal birthweight.BMC Med. 2020 Dec 24;18(1):395. doi: 10.1186/s12916-020-01869-3. BMC Med. 2020. PMID: 33357243 Free PMC article.
-
Cerebral-placental-uterine ratio as novel predictor of late fetal growth restriction: prospective cohort study.Ultrasound Obstet Gynecol. 2019 Sep;54(3):367-375. doi: 10.1002/uog.20150. Ultrasound Obstet Gynecol. 2019. PMID: 30338593
-
Placental Insufficiency in Fetuses That Slow in Growth but Are Born Appropriate for Gestational Age: A Prospective Longitudinal Study.PLoS One. 2016 Jan 5;11(1):e0142788. doi: 10.1371/journal.pone.0142788. eCollection 2016. PLoS One. 2016. PMID: 26730589 Free PMC article.
-
Biochemical tests of placental function versus ultrasound assessment of fetal size for stillbirth and small-for-gestational-age infants.Cochrane Database Syst Rev. 2019 May 14;5(5):CD012245. doi: 10.1002/14651858.CD012245.pub2. Cochrane Database Syst Rev. 2019. PMID: 31087568 Free PMC article.
-
The importance of the cerebroplacental ratio in the evaluation of fetal well-being in SGA and AGA fetuses.Am J Obstet Gynecol. 2015 Jul;213(1):5-15. doi: 10.1016/j.ajog.2015.05.024. Am J Obstet Gynecol. 2015. PMID: 26113227 Review.
Cited by
-
Appropriate-for-gestational-age infants who exhibit reduced antenatal growth velocity display postnatal catch-up growth.PLoS One. 2020 Sep 8;15(9):e0238700. doi: 10.1371/journal.pone.0238700. eCollection 2020. PLoS One. 2020. PMID: 32898169 Free PMC article.
-
Characterization of placental endocrine function and fetal brain development in a mouse model of small for gestational age.Front Endocrinol (Lausanne). 2023 Feb 10;14:1116770. doi: 10.3389/fendo.2023.1116770. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 36843585 Free PMC article.
-
Fetal Growth Velocity-A Breakthrough in Intrauterine Growth Assessment?J Clin Med. 2024 Jun 29;13(13):3842. doi: 10.3390/jcm13133842. J Clin Med. 2024. PMID: 38999408 Free PMC article. Review.
-
Reduced fetal growth velocity precedes antepartum fetal death.Ultrasound Obstet Gynecol. 2021 Jun;57(6):942-952. doi: 10.1002/uog.23111. Ultrasound Obstet Gynecol. 2021. PMID: 32936481 Free PMC article.
-
The ability of continuous-wave Doppler ultrasound to detect fetal growth restriction.PLoS One. 2021 Aug 9;16(8):e0255960. doi: 10.1371/journal.pone.0255960. eCollection 2021. PLoS One. 2021. PMID: 34370790 Free PMC article.
References
-
- Cruz-Martinez R, Savchev S, Cruz-Lemini M, Mendez A, Gratacos E, Figueras F. Clinical utility of third-trimester uterine artery Doppler in the prediction of brain hemodynamic deterioration and adverse perinatal outcome in small-for-gestational-age fetuses. Ultrasound Obstet Gynecol. 2015;45:273–8. doi: 10.1002/uog.14706. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
