

Adaption, implementation and evaluation of collaborative service improvements in the testing and result communication process in primary care from patient and staff perspectives: a qualitative study
- PMID: 28854919
- PMCID: PMC5577659
- DOI: 10.1186/s12913-017-2566-8
Adaption, implementation and evaluation of collaborative service improvements in the testing and result communication process in primary care from patient and staff perspectives: a qualitative study
Abstract
Background: Increasing numbers of blood tests are being ordered in primary care settings and the swift and accurate communication of test results is central to providing high quality care. The process of testing and result communication is complex and reliant on the coordinated actions of care providers, external groups in laboratory and hospital settings, and patients. This fragmentation leaves it vulnerable to error and the need to improve an apparently fallible system is apparent. However, primary care is complex and does not necessarily adopt change in a linear and prescribed manner influenced by a range of factors relating to practice staff, patients and organisational factors. To account for these competing perspectives, we worked in conjunction with both staff and patients to develop and implement strategies intended to improve patient satisfaction and increase efficiency of existing processes.
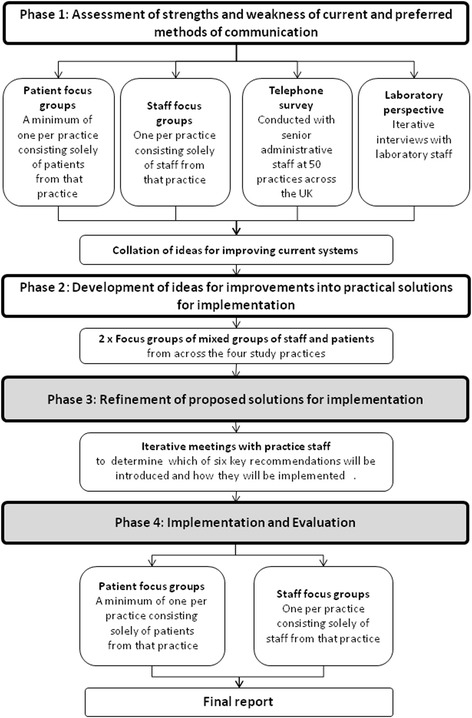
Methods: The study applied the principles of 'experience-based co-design' to identify key areas of weakness and source proposals for change from staff and patients. The study was undertaken within two primary practices situated in South Birmingham (UK) of contrasting size and socio-economic environment. Senior practice staff were involved in the refinement of the interventions for introduction. We conducted focus groups singly constituted of staff and patients at each practice to determine suitability, applicability and desirability alongside the practical implications of their introduction.
Results: At each practice four of the six proposals for change were implemented these were increased access to phlebotomy, improved receptionist training, proactive communication of results, and increased patient awareness of the tests ordered and the means of their communication. All were received favourably by both patients and staff. The remaining issues around the management of telephone calls and the introduction of electronic alerts for missing results were not addressed due to constraints of time and available resources.
Conclusions: Approaches to tackling the same area of weakness differed at practices and was determined by individual staff attitudes and by organisational and patient characteristics. The long-term impact of the changes requires further quantitative evaluation.
Keywords: Clinician-patient communication/relationship; Cllaborative/interdisciplinary care; Healthcare delivery/health services research.
Conflict of interest statement
Authors’ information
RJL is Director of the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) - Birmingham and Black Country and SMG is a Theme Leader. RJM holds an NIHR Professorship and is supported by NIHR Oxford CLAHRC.
Ethics approval and consent to participate
This study was given favourable opinion by the National Research Committee of West Midlands - The Black Country and by the Birmingham and Black Country Comprehensive Local Research Network (REC reference number: 10/H1202/71). All patient and staff participants gave informed consent to participate in the study.
Competing interests
The authors declare they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Patient perspectives on test result communication in primary care: a qualitative study.Br J Gen Pract. 2015 Mar;65(632):e133-40. doi: 10.3399/bjgp15X683929. Br J Gen Pract. 2015. PMID: 25733434 Free PMC article.
-
Routine failures in the process for blood testing and the communication of results to patients in primary care in the UK: a qualitative exploration of patient and provider perspectives.BMJ Qual Saf. 2015 Nov;24(11):681-90. doi: 10.1136/bmjqs-2014-003690. Epub 2015 Aug 6. BMJ Qual Saf. 2015. PMID: 26251507 Free PMC article.
-
Test result communication in primary care: clinical and office staff perspectives.Fam Pract. 2014 Oct;31(5):592-7. doi: 10.1093/fampra/cmu041. Epub 2014 Jul 28. Fam Pract. 2014. PMID: 25070182 Free PMC article.
-
Evidence Brief: Comparative Effectiveness of Appointment Recall Reminder Procedures for Follow-up Appointments [Internet].Washington (DC): Department of Veterans Affairs (US); 2015 Jul. Washington (DC): Department of Veterans Affairs (US); 2015 Jul. PMID: 27606388 Free Books & Documents. Review.
-
Why do acute healthcare staff behave unprofessionally towards each other and how can these behaviours be reduced? A realist review.Health Soc Care Deliv Res. 2024 Aug;12(25):1-195. doi: 10.3310/PAMV3758. Health Soc Care Deliv Res. 2024. PMID: 39239681 Review.
Cited by
-
Patient facing decision support system for interpretation of laboratory test results.BMC Med Inform Decis Mak. 2018 Jul 20;18(1):68. doi: 10.1186/s12911-018-0648-0. BMC Med Inform Decis Mak. 2018. PMID: 30029644 Free PMC article.
-
Quality improvements of safety-netting guidelines for cancer in UK primary care: insights from a qualitative interview study of GPs.Br J Gen Pract. 2019 Nov 28;69(689):e819-e826. doi: 10.3399/bjgp19X706565. Print 2019 Dec. Br J Gen Pract. 2019. PMID: 31685542 Free PMC article.
-
Communicating blood test results in primary care: a mixed-methods systematic review.Br J Gen Pract. 2025 Mar 27;75(753):e222-e231. doi: 10.3399/BJGP.2024.0338. Print 2025 Apr. Br J Gen Pract. 2025. PMID: 39374979 Free PMC article.
-
Measurement and outcomes of co-production in health and social care: a systematic review of empirical studies.BMJ Open. 2023 Sep 22;13(9):e073808. doi: 10.1136/bmjopen-2023-073808. BMJ Open. 2023. PMID: 37739472 Free PMC article.
-
Patients and Healthcare Providers' Perspectives on Patient Experience Factors and a Model of Patient-Centered Care Communication: A Systematic Review.Healthcare (Basel). 2024 May 26;12(11):1090. doi: 10.3390/healthcare12111090. Healthcare (Basel). 2024. PMID: 38891165 Free PMC article. Review.
References
-
- Hickner J, Graham DG, Elder NC, Brandt E, Emsermann CB, Dovey S, et al. Testing process errors and their harms and consequences reported from family medicine practices: a study of the American Academy of family physicians National Research Network. Qual Saf Health Car. 2008;17:194–200. doi: 10.1136/qshc.2006.021915. - DOI - PubMed
-
- Elder NC, McEwen TR, Flach JM, Gallimore JJ. Creating safety in the testing process in primary care offices. In: Henriksen K, Battles JB, Keyes MA, Grady ML, editors. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 2: Culture and Redesign) Rockville, MD: Agency for Healthcare Research and Quality (US); 2008. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
