

The effectiveness of multidisciplinary care models for patients with chronic kidney disease: a systematic review and meta-analysis
- PMID: 28856498
- PMCID: PMC5811573
- DOI: 10.1007/s11255-017-1679-7
The effectiveness of multidisciplinary care models for patients with chronic kidney disease: a systematic review and meta-analysis
Abstract
Aim: To assess the efficacy of the multidisciplinary care (MDC) model for patients with chronic kidney disease (CKD).
Background: The MDC model has been used in clinical practice for years, but the effectiveness of the MDC model for patients with CKD remains controversial.
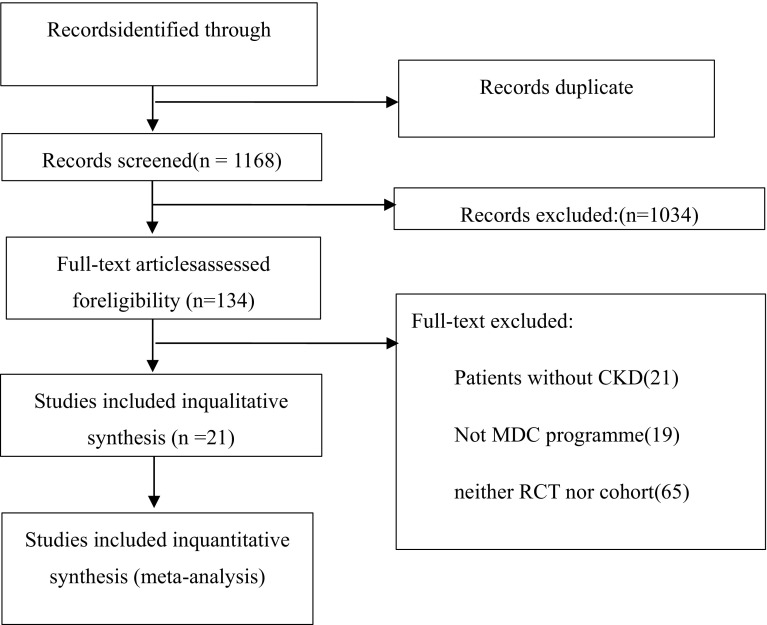
Methods: Embase, PubMed, Medline, the Cochrane Library, and China National Knowledge Infrastructure databases were used to search for relevant articles. Only randomized controlled trials and cohort studies were pooled. Two independent authors assessed all articles and extracted the data. The efficacy was estimated from the odds ratios and corresponding 95% confidence intervals. A random effects model was used according to the heterogeneity.
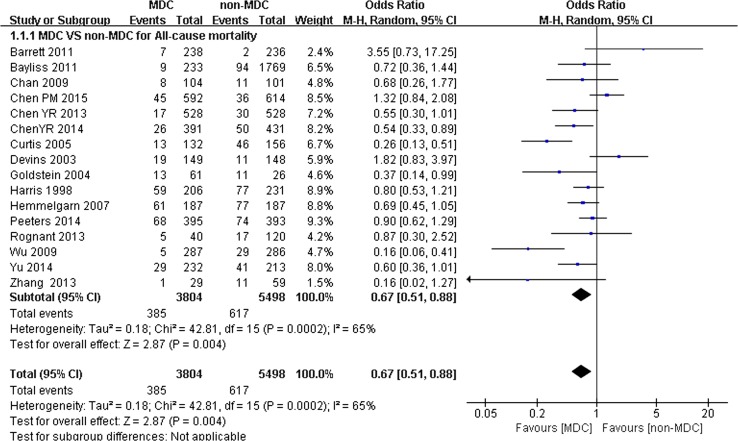
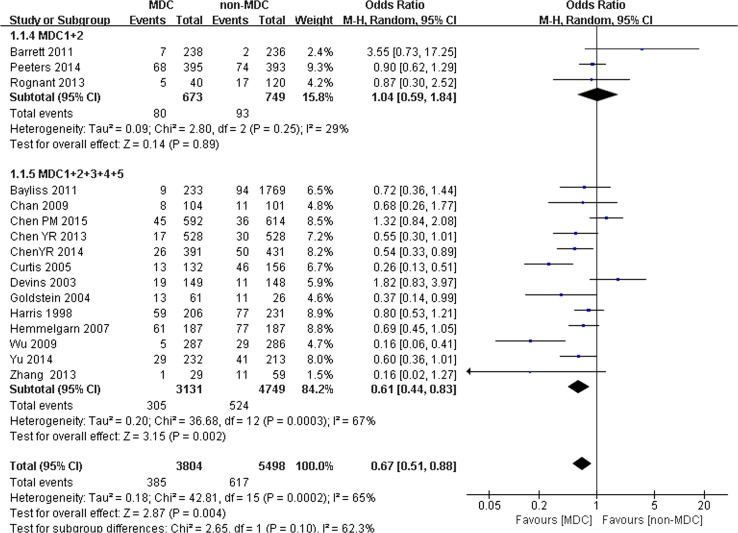
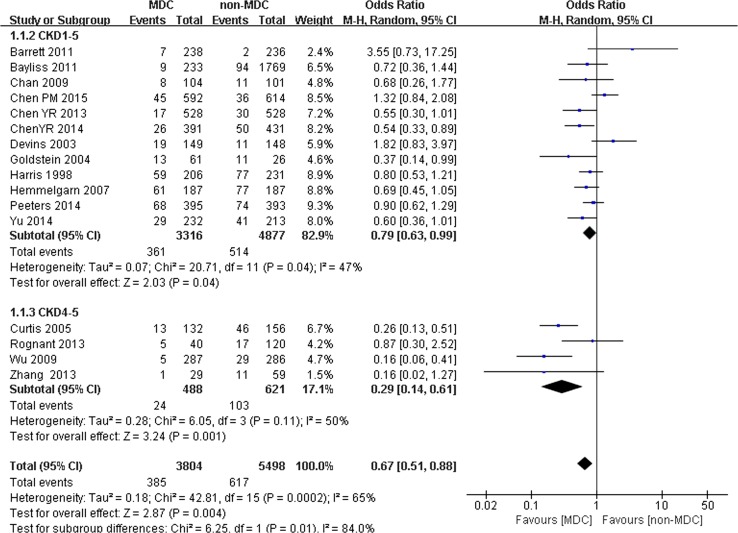
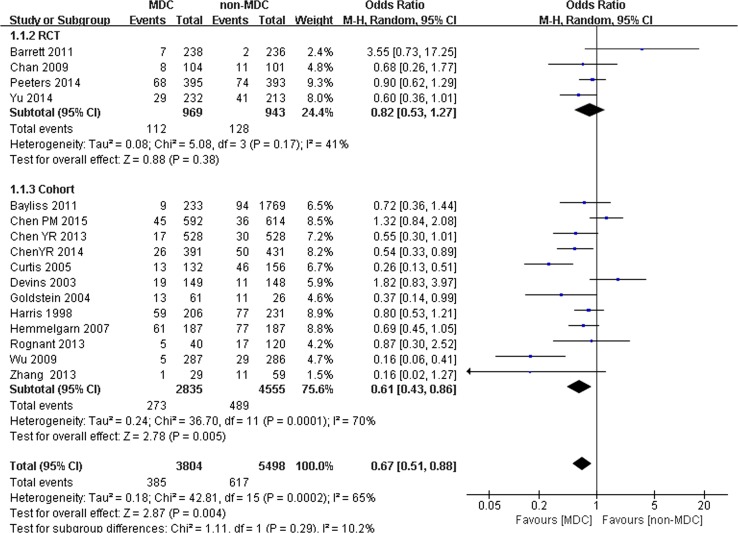
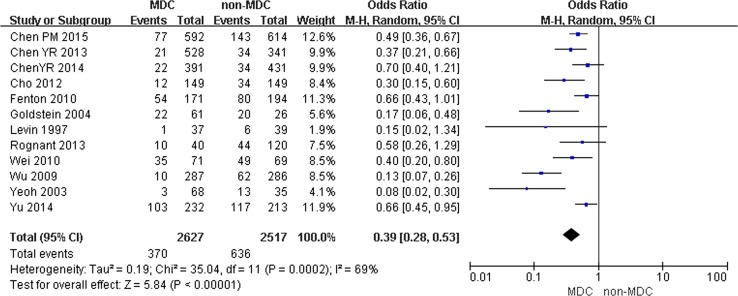
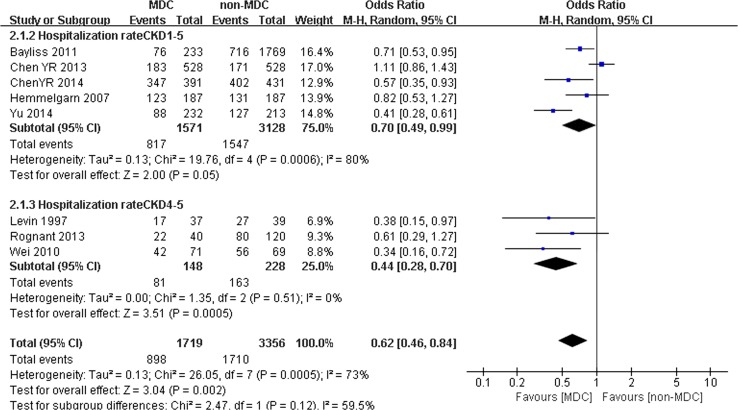
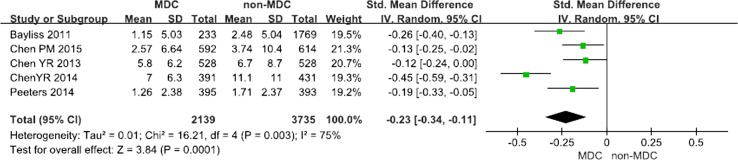
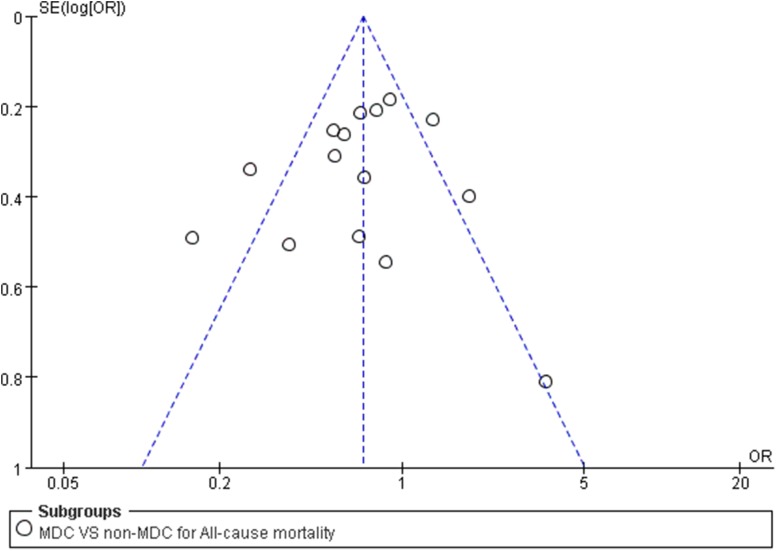
Results: Twenty-one studies including 10,284 participants were analyzed. Compared with the non-MDC group, MDC was associated with a lower risk of all-cause mortality and lower hospitalization rates for patients with CKD. In addition, MDC also resulted in a slower eGFR decline and reduced temporary catheterization for patients receiving dialysis. However, according to the subgroup analysis, the lower rates of all-cause mortality in the MDC group were observed only in patients in stage 4-5 and when the staff of the MDC consisted of nephrologists, nurse specialists and professionals from other fields. The most prominent effect of reducing the hospitalization rates was also observed in patients with stage 4-5 but not in patients with stage 4-5 CKD.
Conclusions: MDC can lower the all-cause mortality of patients with CKD, reduce temporary catheterization for patients receiving dialysis, decrease the hospitalization rate, and slow the eGFR decline. Moreover, the reduction in all-cause mortality crucially depends on the professionals comprising the MDC staff and the stage of CKD in patients. In addition, the CKD stage influences the hospitalization rates.
Keywords: Care; Chronic kidney disease; Multidisciplinary; Systematic reviews and meta-analysis.
Conflict of interest statement
Conflict of interest
The authors have no interest conflicts regarding this study.
Availability of data and material
Embase, PubMed, Medline, the Cochrane Library, and China National Knowledge Infrastructure (CNKI) databases were used to identify all relevant published articles for review. These articles are open to the public.
Ethical standard
In accordance with the ethical standards of institutional and international research committee, this article is based on previous published studies; thus, it does not contain any studies with human participants or animals.
Figures
Comment in
-
Living Kidney Donation Between African Immigrants.Prog Transplant. 2023 Dec;33(4):360-362. doi: 10.1177/15269248231212909. Epub 2023 Nov 14. Prog Transplant. 2023. PMID: 37964550 No abstract available.
References
-
- National Kidney F. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
