

The Treatment Effect of an ACE-Inhibitor Based Regimen with Perindopril in Relation to Beta-Blocker use in 29,463 Patients with Vascular Disease: a Combined Analysis of Individual Data of ADVANCE, EUROPA and PROGRESS Trials
- PMID: 28856537
- PMCID: PMC5607906
- DOI: 10.1007/s10557-017-6747-9
The Treatment Effect of an ACE-Inhibitor Based Regimen with Perindopril in Relation to Beta-Blocker use in 29,463 Patients with Vascular Disease: a Combined Analysis of Individual Data of ADVANCE, EUROPA and PROGRESS Trials
Abstract
Introduction: In everyday practice, angiotensin converting enzyme inhibitors and beta-blockers are cornerstone treatments in patients with (cardio-)vascular disease. Clear data that evaluate the effects of the combination of these agents on morbidity and mortality are lacking.
Methods: In this retrospective pooled analysis of three large perindopril outcome trials (ADVANCE, EUROPA, PROGRESS), clinical outcomes were evaluated in 29,463 patients with vascular disease. Multivariate Cox regression analyses were performed in patients randomized to a perindopril-based regimen or placebo (treatment effect), and data were stratified according to background beta-blocker treatment. The primary endpoint was a composite of cardiovascular mortality, non-fatal myocardial infarction, and stroke.
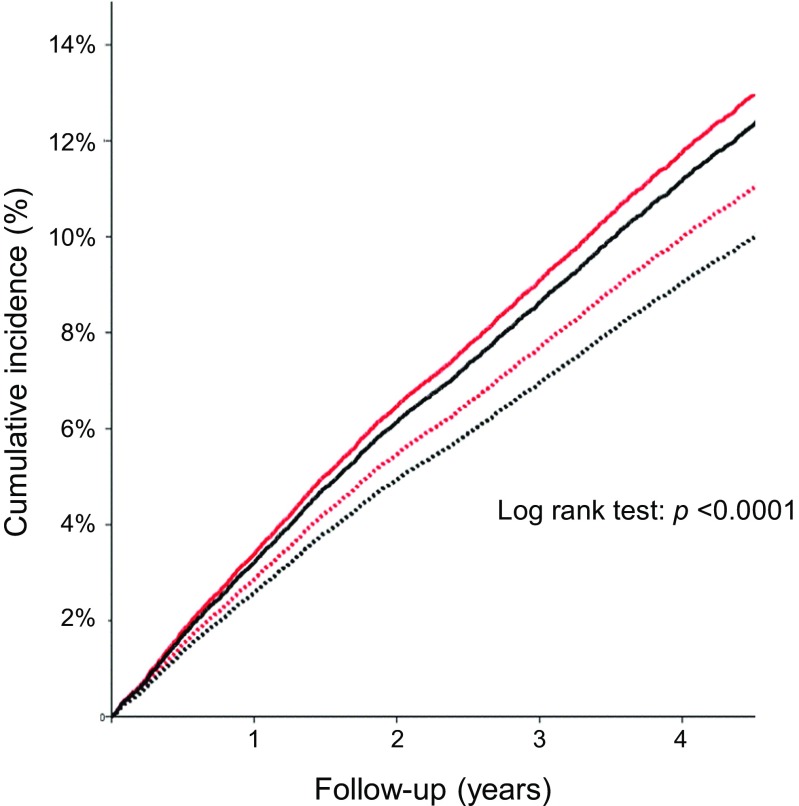
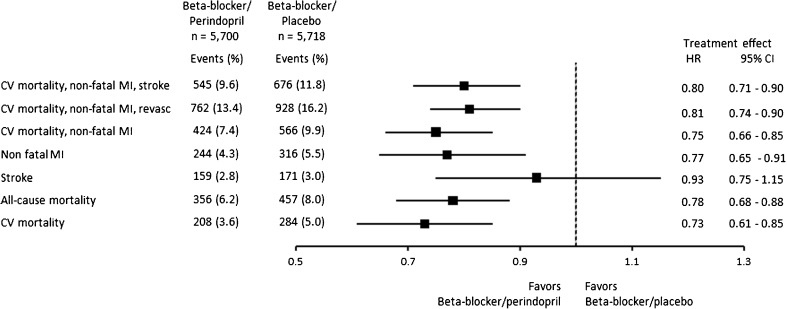
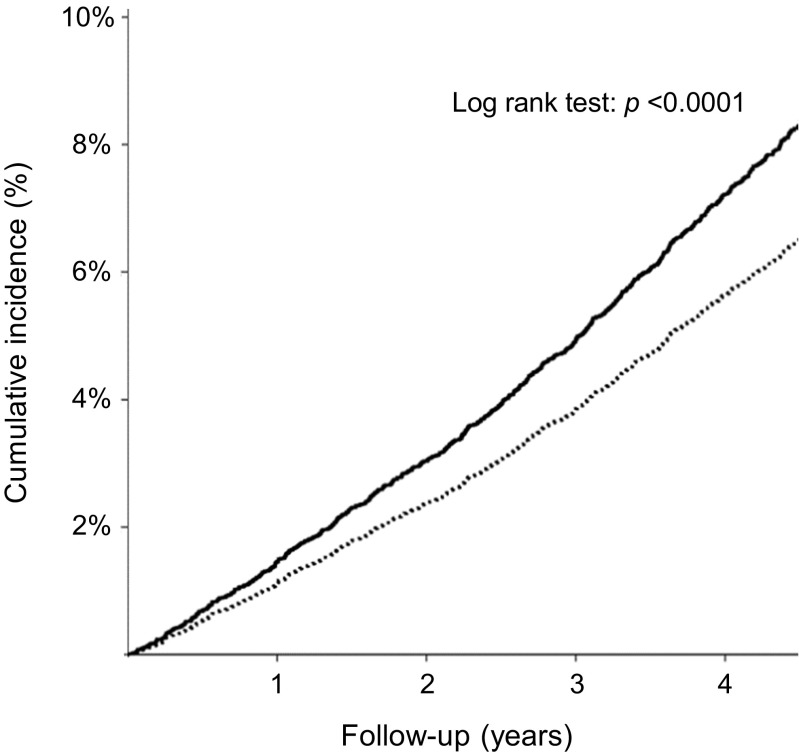
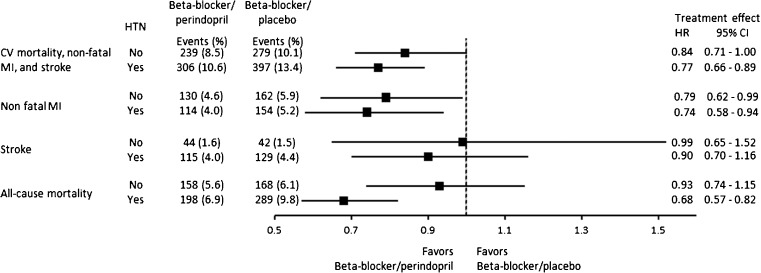
Results: The cumulative incidence of the primary endpoint over mean follow-up of 4.0 years (Sd 1.0) was significantly lower in the beta-blocker/perindopril group (9.6%; 545/5700 patients) as compared to beta-blocker/placebo (11.8%; 676/5718 patients) (p < 0.01). Adding perindopril to existing beta-blocker treatment reduced the relative risk of the primary endpoint by 20% (hazard ratio (HR) 0.80; 95% confidence interval (CI) 0.71-0.90), non-fatal myocardial infarction by 23% (HR 0.77; 95% CI 0.65-0.91), and all-cause mortality by 22% (HR 0.78; 95% CI 0.68-0.88) as compared to placebo. Significant treatment benefit was not observed for stroke (HR 0.93; 95% CI 0.75-1.15). Significance was maintained for the primary endpoint and cardiovascular endpoints when data were further stratified by baseline hypertension. However, the mortality benefit was only observed in patients with hypertension with background beta-blocker use.
Conclusions: These data suggest that the beneficial cardioprotective effects of perindopril treatment are additive to the background beta-blockers use.
Keywords: ACE-inhibitor; Beta-blocker; Hypertension; Perindopril; Prevention; Vascular disease.
Conflict of interest statement
J.B., J.C., S.M., K.F., R.F., W.R. M.L.S., and E.B. have received research grants and fees from Servier.
Figures
References
-
- Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) J Hypertens. 2013;31(7):1281–1357. - PubMed
-
- Rosendorff C, Lackland DT, Allison M, Aronow WS, Black HR, Blumenthal RS, et al. Treatment of hypertension in patients with coronary artery disease: a scientific statement from the American Heart Association, American College of Cardiology, and American Society of Hypertension. J Am Coll Cardiol. 2015;65(18):1998–2038. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. - PubMed
-
- Thoenes M, Neuberger HR, Volpe M, Khan BV, Kirch W, Bohm M. Antihypertensive drug therapy and blood pressure control in men and women: an international perspective. J Hum Hypertens. 2010;24(5):336–344. - PubMed
-
- Kotseva K, Wood D, De Bacquer D, De Backer G, Ryden L, Jennings C, et al. EUROASPIRE IV: a European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur J Prev Cardiol. 2016;23(6):636–648. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
