

Disparities in hypertension and cardiovascular disease in blacks: The critical role of medication adherence
- PMID: 28856834
- PMCID: PMC5638710
- DOI: 10.1111/jch.13089
Disparities in hypertension and cardiovascular disease in blacks: The critical role of medication adherence
Abstract
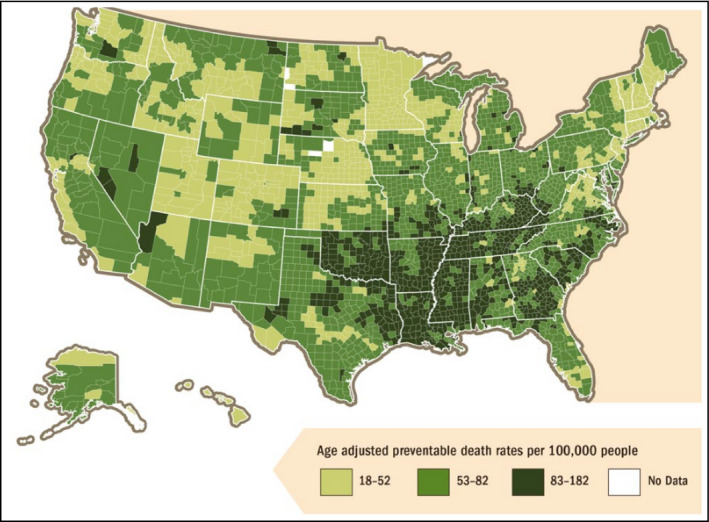
Blacks are two to three times as likely as whites to die of preventable heart disease and stroke. Declines in mortality from heart disease have not eliminated racial disparities. Control and effective treatment of hypertension, a leading cause of cardiovascular disease, among blacks is less than in whites and remains a challenge. One of the driving forces behind this racial/ethnic disparity is medication nonadherence whose cause is embedded in social determinants. Eight practical approaches to addressing medication adherence with the potential to attenuate disparities were identified and include: (1) patient engagement strategies, (2) consumer-directed health care, (3) patient portals, (4) smart apps and text messages, (5) digital pillboxes, (6) pharmacist-led engagement, (7) cardiac rehabilitation, and (8) cognitive-based behavior. However, while data suggest that these strategies may improve medication adherence, the effect on ameliorating racial/ethnic disparities is not certain. This review describes the relationship between disparities and medication adherence, which likely plays a role in persistent disparities in cardiovascular morbidity and mortality.
Keywords: Adherence; Food and Drug Administration; blacks; cardiovascular disease; health disparities; hypertension; race/ethnicity.
©2017 Wiley Periodicals, Inc.
Conflict of interest statement
Dr Cryer serves as consultant for Esperion Therapeutics. Dr Ferdinand received a grant from Boehringer Ingleheim and serves as consultant for Amgen, Sanofi, Boehringer Ingleheim, Quantum Genomics, Novartis, and Eli Lily. Drs Senatore, Clayton‐Jeter, Lewin, Nasser, and Yadav have nothing to disclose.
Figures
Comment in
-
Reexamining medication adherence in black patients with hypertension through the lens of the social determinants of health.J Clin Hypertens (Greenwich). 2017 Oct;19(10):1025-1027. doi: 10.1111/jch.13071. Epub 2017 Sep 24. J Clin Hypertens (Greenwich). 2017. PMID: 28942605 Free PMC article. No abstract available.
References
-
- Ritchey M, Chang A, Powers C, et al. Vital signs: disparities in antihypertensive medication nonadherence among Medicare part D beneficiaries—United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65:967‐976. - PubMed
-
- Flack JM, Sica DA, Bakris G, et al. International Society on Hypertension in Blacks. Management of high blood pressure in blacks: an update of the International Society on Hypertension in Blacks consensus statement. Hypertension. 2010;56:780‐800. - PubMed
-
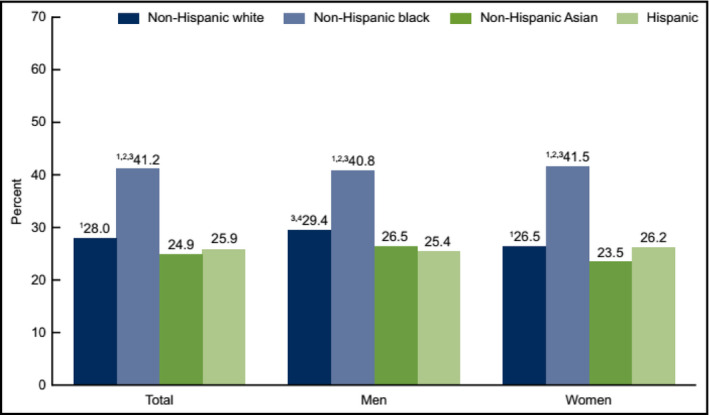
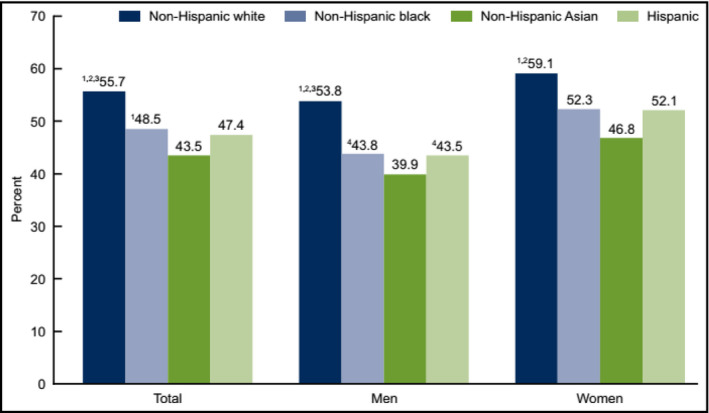
- Yoon SS, Carroll MD, Fryar CD. Hypertension prevalence and control among adults: United States, 2011–2014. NCHS Data Brief. 2015;(220):1‐8. - PubMed
-
- Havranek EP, Mujahid MS, Barr DA, et al. Social determinants of risk and outcomes for cardiovascular disease. Circulation. 2015;132:873‐898. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
