

Fusions in solid tumours: diagnostic strategies, targeted therapy, and acquired resistance
- PMID: 28857077
- PMCID: PMC10452928
- DOI: 10.1038/nrclinonc.2017.127
Fusions in solid tumours: diagnostic strategies, targeted therapy, and acquired resistance
Abstract
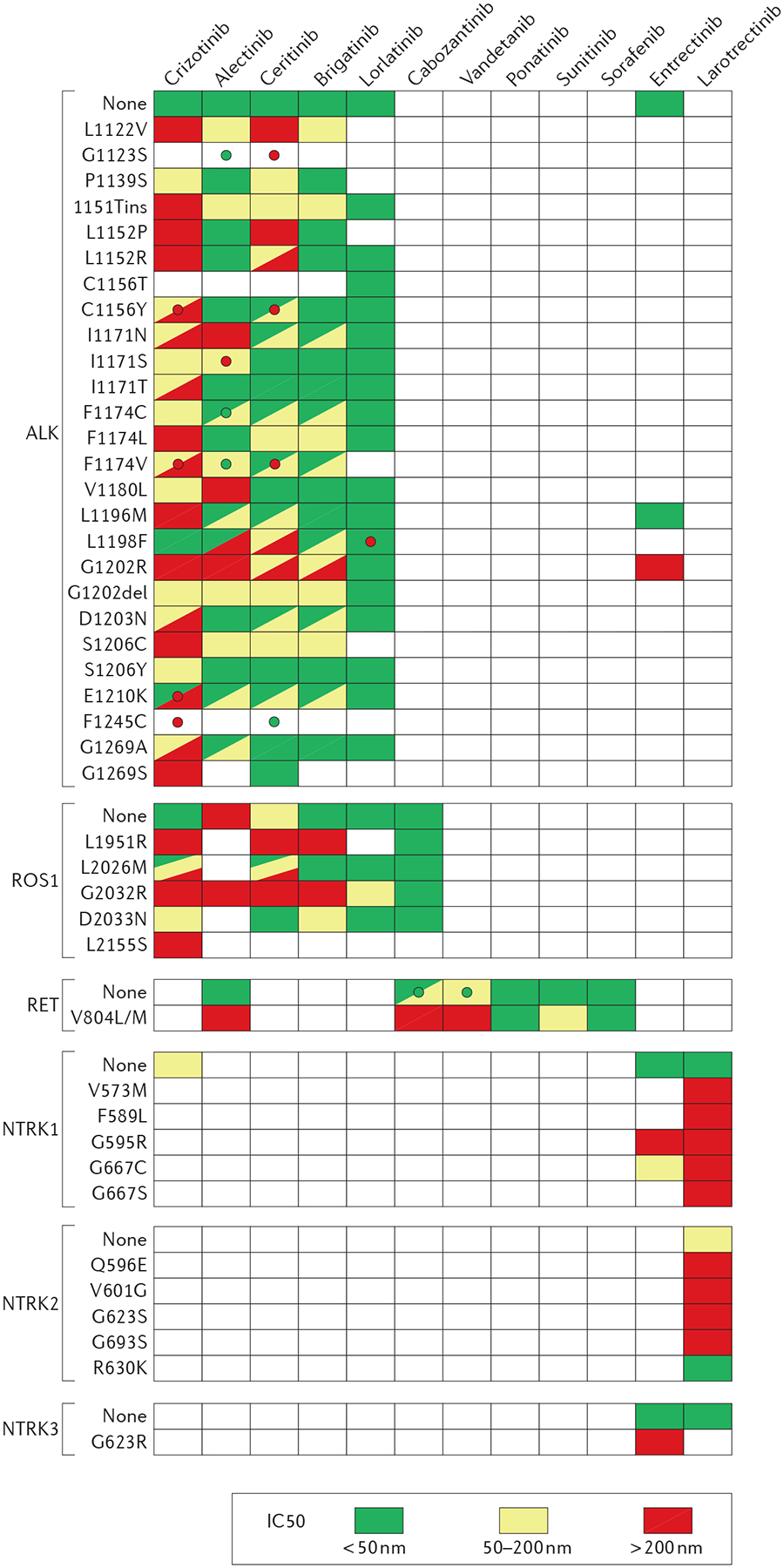
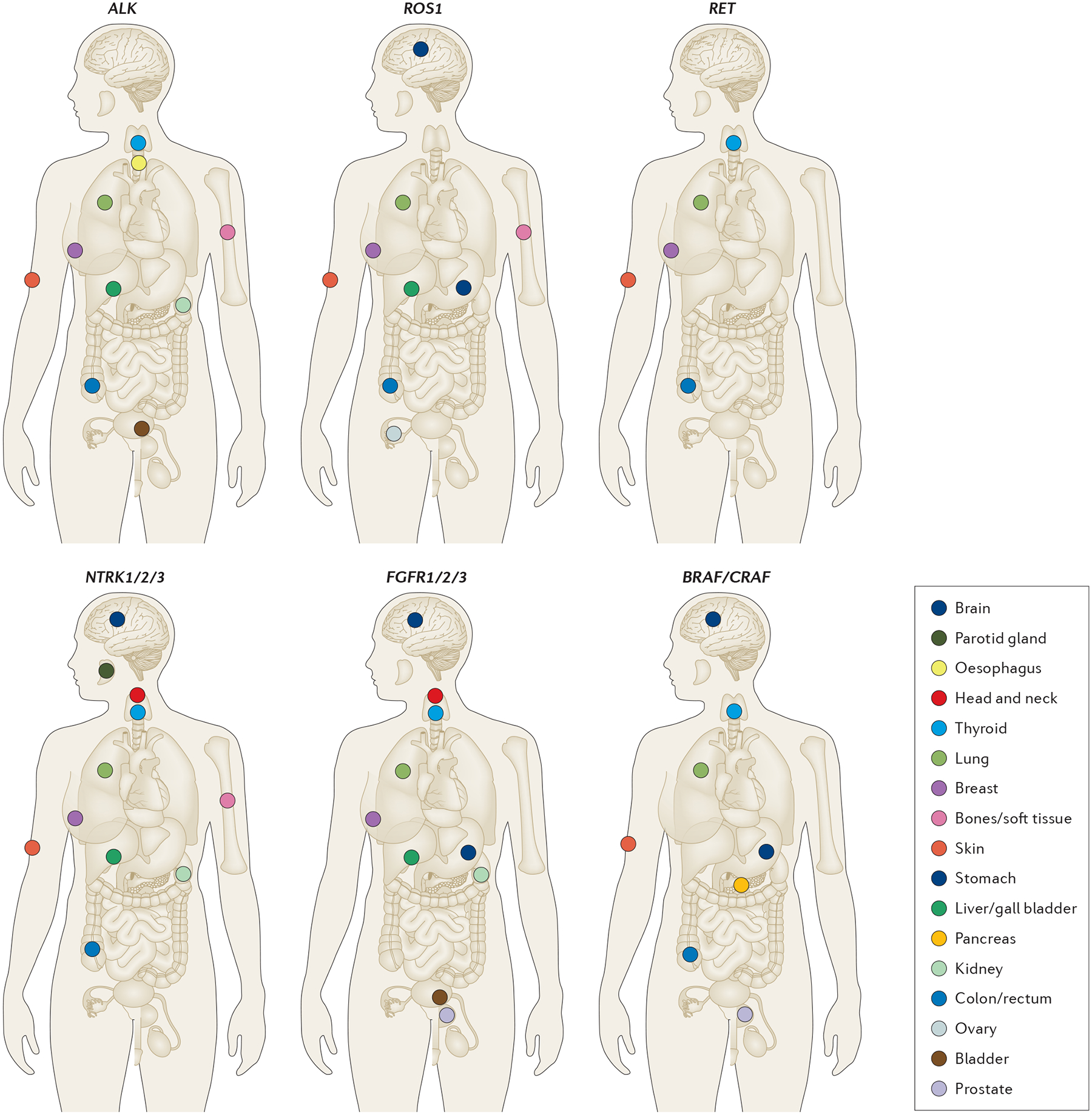
Structural gene rearrangements resulting in gene fusions are frequent events in solid tumours. The identification of certain activating fusions can aid in the diagnosis and effective treatment of patients with tumours harbouring these alterations. Advances in the techniques used to identify fusions have enabled physicians to detect these alterations in the clinic. Targeted therapies directed at constitutively activated oncogenic tyrosine kinases have proven remarkably effective against cancers with fusions involving ALK, ROS1, or PDGFB, and the efficacy of this approach continues to be explored in malignancies with RET, NTRK1/2/3, FGFR1/2/3, and BRAF/CRAF fusions. Nevertheless, prolonged treatment with such tyrosine-kinase inhibitors (TKIs) leads to the development of acquired resistance to therapy. This resistance can be mediated by mutations that alter drug binding, or by the activation of bypass pathways. Second-generation and third-generation TKIs have been developed to overcome resistance, and have variable levels of activity against tumours harbouring individual mutations that confer resistance to first-generation TKIs. The rational sequential administration of different inhibitors is emerging as a new treatment paradigm for patients with tumours that retain continued dependency on the downstream kinase of interest.
Conflict of interest statement
Competing interests statement
A.D. has received honoraria from and is an advisory board member for Ariad, AstraZeneca, Blueprint Medicines, Exelixis, Genentech/Roche, Ignyta and Loxo Oncology and has received research funding from Foundation Medicine. The other authors declare no competing interests.
Figures
References
-
- Mitelman F, Johansson B & Mertens F The impact of translocations and gene fusions on cancer causation. Nat. Rev. Cancer 7, 233–245 (2007). - PubMed
-
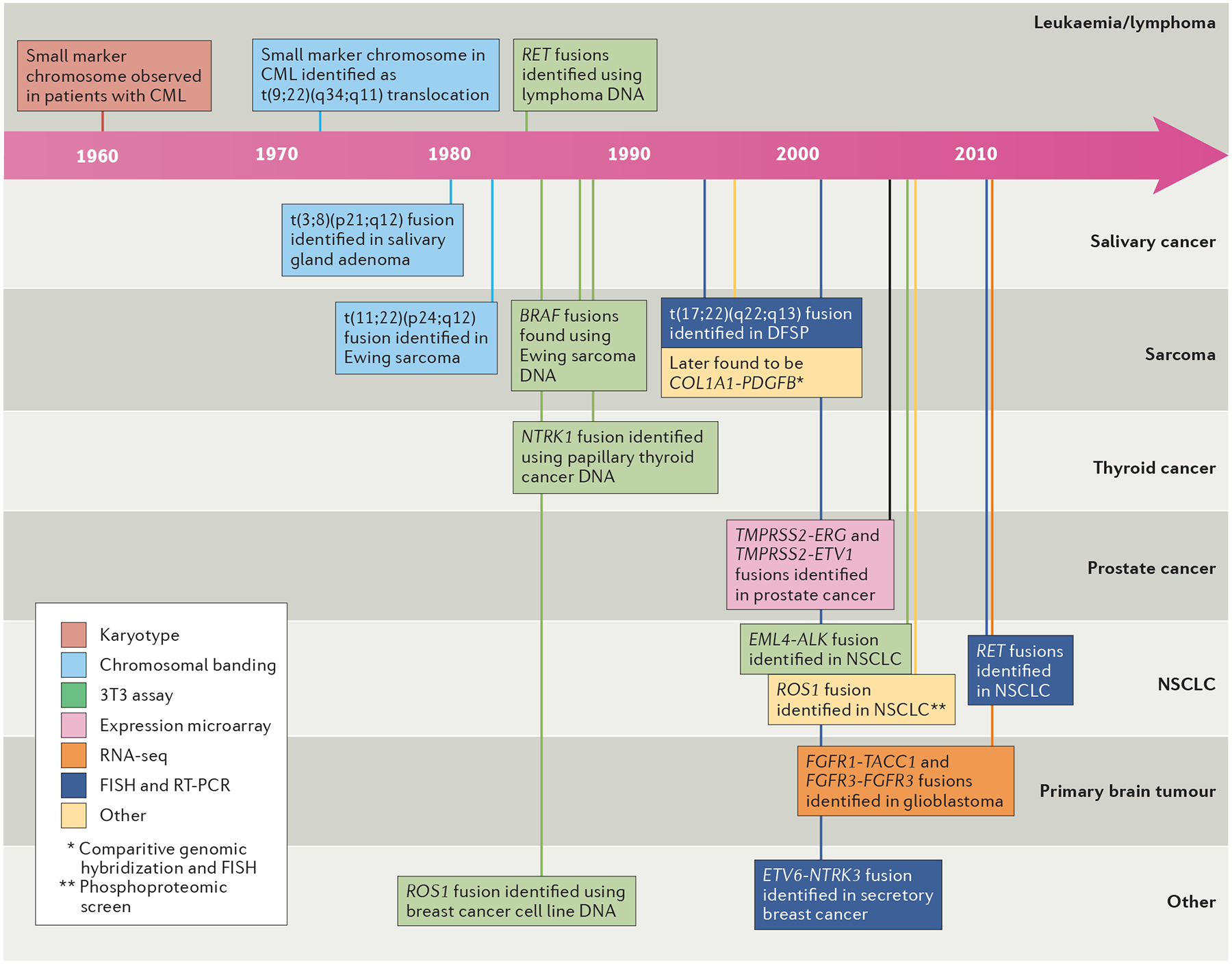
- Nowell P & Hungerford D Minute chromosome in human chronic granulocytic leukemia. Science 132, 1497–1497 (1960).
-
- Rowley JD A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature 243, 290–293 (1973). - PubMed
-
- Mertens F, Johansson B, Fioretos T & Mitelman F The emerging complexity of gene fusions in cancer. Nat. Rev. Cancer 15, 371–381 (2015). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
