

Age at Exposure to Surgery and Anesthesia in Children and Association With Mental Disorder Diagnosis
- PMID: 28857799
- PMCID: PMC5856466
- DOI: 10.1213/ANE.0000000000002423
Age at Exposure to Surgery and Anesthesia in Children and Association With Mental Disorder Diagnosis
Abstract
Background: Animals exposed to anesthetics during specific age periods of brain development experience neurotoxicity, with neurodevelopmental changes subsequently observed during adulthood. The corresponding vulnerable age in children, however, is unknown.
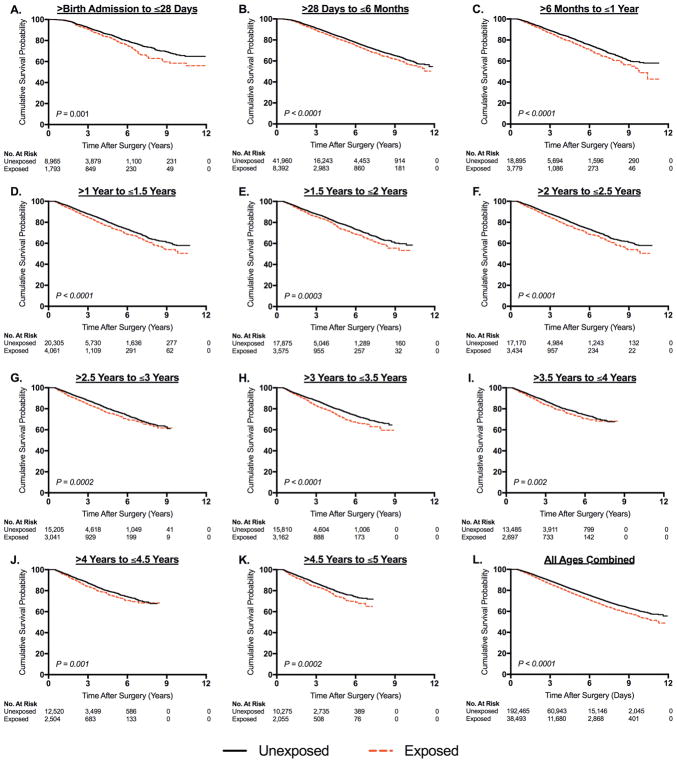
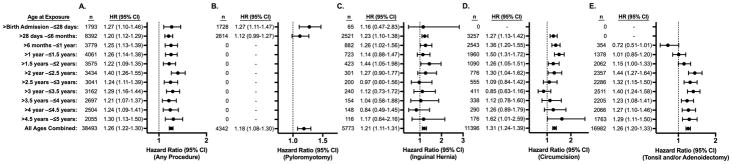
Methods: An observational cohort study was performed using a longitudinal dataset constructed by linking individual-level Medicaid claims from Texas and New York from 1999 to 2010. This dataset was evaluated to determine whether the timing of exposure to anesthesia ≤5 years of age for a single common procedure (pyloromyotomy, inguinal hernia, circumcision outside the perinatal period, or tonsillectomy and/or adenoidectomy) is associated with increased subsequent risk of diagnoses for any mental disorder, or specifically developmental delay (DD) such as reading and language disorders, and attention deficit hyperactivity disorder (ADHD). Exposure to anesthesia and surgery was evaluated in 11 separate age at exposure categories: ≤28 days old, >28 days and ≤6 months, >6 months and ≤1 year, and 6-month age intervals between >1 year old and ≤5 years old. For each exposed child, 5 children matched on propensity score calculated using sociodemographic and clinical covariates were selected for comparison. Cox proportional hazards models were used to measure the hazard ratio of a mental disorder diagnosis associated with exposure to surgery and anesthesia.
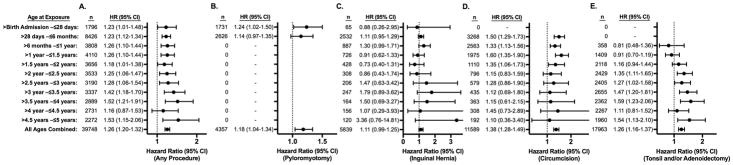
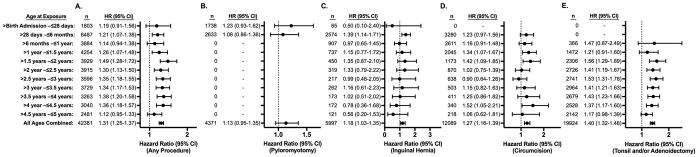
Results: A total of 38,493 children with a single exposure and 192,465 propensity score-matched children unexposed before 5 years of age were included in the analysis. Increased risk of mental disorder diagnosis was observed at all ages at exposure with an overall hazard ratio of 1.26 (95% confidence interval [CI], 1.22-1.30), which did not vary significantly with the timing of exposure. Analysis of DD and ADHD showed similar results, with elevated hazard ratios distributed evenly across all ages, and overall hazard ratios of 1.26 (95% CI, 1.20-1.32) for DD and 1.31 (95% CI, 1.25-1.37) for ADHD.
Conclusions: Children who undergo minor surgery requiring anesthesia under age 5 have a small but statistically significant increased risk of mental disorder diagnoses and DD and ADHD diagnoses, but the timing of the surgical procedure does not alter the elevated risks. Based on these findings, there is little support for the concept of delaying a minor procedure to reduce long-term neurodevelopmental risks of anesthesia in children. In evaluating the influence of age at exposure, the types of procedures included may need to be considered, as some procedures are associated with specific comorbid conditions and are only performed at certain ages.
Conflict of interest statement
Figures
Comment in
-
Association of Surgery and Anesthesia With Mental Disorder Diagnoses: What Would Sir Austin Bradford Hill Say?Anesth Analg. 2017 Dec;125(6):1845-1848. doi: 10.1213/ANE.0000000000002567. Anesth Analg. 2017. PMID: 29189364 Free PMC article. No abstract available.
-
Further Study Needed of the Impact of Early-Life Surgery With Associated General Anesthesia on the Risk of Attention Deficit Hyperactivity Disorder.Anesth Analg. 2021 Mar 1;132(3):e46-e47. doi: 10.1213/ANE.0000000000005341. Anesth Analg. 2021. PMID: 33591104 No abstract available.
-
In Response.Anesth Analg. 2021 Mar 1;132(3):e47-e48. doi: 10.1213/ANE.0000000000005342. Anesth Analg. 2021. PMID: 33591105 No abstract available.
References
-
- Jevtovic-Todorovic V, Hartman RE, Izumi Y, Benshoff ND, Dikranian K, Zorumski CF, Olney JW, Wozniak DF. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. Journal of Neuroscience. 2003;23:876–82. - PMC - PubMed
-
- Zou X, Liu F, Zhang X, Patterson TA, Callicott R, Liu S, Hanig JP, Paule MG, Slikker W, Jr, Wang C. Inhalation anesthetic-induced neuronal damage in the developing rhesus monkey. Neurotoxicol Teratol. 2011;33:592–7. - PubMed
-
- Loepke AW, Soriano SG. An assessment of the effects of general anesthetics on developing brain structure and neurocognitive function. Anesth Analg. 2008;106:1681–707. - PubMed
-
- Disma N, Mondardini MC, Terrando N, Absalom AR, Bilotta F. A systematic review of methodology applied during preclinical anesthetic neurotoxicity studies: important issues and lessons relevant to the design of future clinical research. Paediatr Anaesth. 2016;26:6–36. - PubMed
-
- Casey BJ, Tottenham N, Liston C, Durston S. Imaging the developing brain: what have we learned about cognitive development? Trends Cogn Sci. 2005;9:104–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
